
3FWJFX SUJDMF …downloads.hindawi.com/journals/tswj/2013/427817.pdf · dpnqmfujpo espq pvu...
23
Hindawi Publishing Corporation e Scienti�c World �ournal Volume 2013, Article ID 427817, 22 pages http://dx.doi.org/10.1155/2013/427817 Review Article Therapeutic Communities for Addictions: A Review of Their Effectiveness from a Recovery-Oriented Perspective Wouter Vanderplasschen, 1 Kathy Colpaert, 1 Mieke Autrique, 1 Richard Charles Rapp, 2 Steve Pearce, 3 Eric Broekaert, 1 and Stijn Vandevelde 4 1 Department of Orthopedagogics, Ghent University, H. Dunantlaan 2, 9000 Ghent, Belgium 2 Boonsho School of Medicine, Center for Interventions, Treatment and Addictions Research (CITAR), Wright State University, 3640 Colonel Glenn Highway, Dayton, OH 45435, USA 3 Oxfordshire Complex Needs Service, Oxfordshire and Buckinghamshire Mental Health NHS Foundation Trust, Manzil Way, Oxford OX4 1XE, UK 4 Faculty of Education, Health and Social Work, University College Ghent, 9000 Ghent, Belgium Correspondence should be addressed to Wouter Vanderplasschen; [email protected] Received 28 October 2012; Accepted 9 December 2012 Academic Editors: V. Di Michele, S. M. Dursun, and T. Shioiri Copyright © 2013 Wouter Vanderplasschen et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. erapeutic communities (TCs) for addictions are drug-free environments in which people with addictive problems live together in an organized and structured way to promote change toward recovery and reinsertion in society. Despite a long research tradition in TCs, the evidence base for the effectiveness of TCs is limited according to available reviews. Since most of these studies applied a selective focus, we made a comprehensive systematic review of all controlled studies that compared the effectiveness of TCs for addictions with that of a control condition. e focus of this paper is on recovery, including attention for various life domains and a longitudinal scope. We searched the following databases: ISI Web of Knowledge (WoS), PubMed, and DrugScope. Our search strategy revealed 997 hits. Eventually, 30 publications were selected for this paper, which were based on 16 original studies. Two out of three studies showed signi�cantly better substance use and legal outcomes among TC participants, and �ve studies found superior employment and psychological functioning. Length of stay in treatment and participation in subsequent aercare were consistent predictors of recovery status. We conclude that TCs can promote change regarding various outcome categories. Since recovering addicts oen cycle between abstinence and relapse, a continuing care approach is advisable, including assessment of multiple and subjective outcome indicators. 1. Introduction Drug addiction is a complex mental health problem that is oen associated with difficulties in various life domains such as unemployment, homelessness, relational con�icts, problems with the courts, and psychiatric comorbidity [1, 2]. While some of these problems certainly evolve from the abuse of substances, many eventual addicts suffer from these problems prior to the onset of their drug use [3]. In both cases, drug addiction has generally been treated as an acute condition during brief episodes of residential care or several months of outpatient treatment, where the primary if not exclusive focus has been on abstinence to the exclusion of other concerns [4]. In contrast, addiction is increasingly regarded as a chronic relapsing disorder where recovery is possible [5], but oen the one that requires intensive or even multiple treatment episodes and/or strong personal or community resources. A continuing care approach is needed to initiate and maintain recovery [6, 7]. e recov- ery movement focuses on individuals’ perceived needs and objectives and sees abstinence as a potential resource, but not as a prerequisite, for recovery [8–10]. A recovery-oriented approach in addiction research implies attention for the evolutions on various life domains and individuals’ subjective
Transcript of 3FWJFX SUJDMF …downloads.hindawi.com/journals/tswj/2013/427817.pdf · dpnqmfujpo espq pvu...

Hindawi Publishing Corporatione Scienti�c World �ournalVolume 2013, Article ID 427817, 22 pageshttp://dx.doi.org/10.1155/2013/427817
Review ArticleTherapeutic Communities for Addictions: A Review ofTheir Effectiveness from a Recovery-Oriented Perspective
Wouter Vanderplasschen,1 Kathy Colpaert,1 Mieke Autrique,1 Richard Charles Rapp,2
Steve Pearce,3 Eric Broekaert,1 and Stijn Vandevelde4
1 Department of Orthopedagogics, Ghent University, H. Dunantlaan 2, 9000 Ghent, Belgium2Boonsho School of Medicine, Center for Interventions, Treatment and Addictions Research (CITAR), Wright State University,3640 Colonel Glenn Highway, Dayton, OH 45435, USA
3Oxfordshire Complex Needs Service, Oxfordshire and Buckinghamshire Mental Health NHS Foundation Trust, Manzil Way,Oxford OX4 1XE, UK
4 Faculty of Education, Health and Social Work, University College Ghent, 9000 Ghent, Belgium
Correspondence should be addressed to Wouter Vanderplasschen; [email protected]
Received 28 October 2012; Accepted 9 December 2012
Academic Editors: V. Di Michele, S. M. Dursun, and T. Shioiri
Copyright © 2013 Wouter Vanderplasschen et al. is is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
erapeutic communities (TCs) for addictions are drug-free environments in which people with addictive problems live togetherin an organized and structured way to promote change toward recovery and reinsertion in society. Despite a long research traditionin TCs, the evidence base for the effectiveness of TCs is limited according to available reviews. Since most of these studies applieda selective focus, we made a comprehensive systematic review of all controlled studies that compared the effectiveness of TCs foraddictions with that of a control condition. e focus of this paper is on recovery, including attention for various life domains anda longitudinal scope. We searched the following databases: ISI Web of Knowledge (WoS), PubMed, and DrugScope. Our searchstrategy revealed 997 hits. Eventually, 30 publications were selected for this paper, which were based on 16 original studies. Twoout of three studies showed signi�cantly better substance use and legal outcomes among TC participants, and �ve studies foundsuperior employment and psychological functioning. Length of stay in treatment and participation in subsequent aercare wereconsistent predictors of recovery status. We conclude that TCs can promote change regarding various outcome categories. Sincerecovering addicts oen cycle between abstinence and relapse, a continuing care approach is advisable, including assessment ofmultiple and subjective outcome indicators.
1. Introduction
Drug addiction is a complex mental health problem thatis oen associated with difficulties in various life domainssuch as unemployment, homelessness, relational con�icts,problems with the courts, and psychiatric comorbidity [1, 2].While some of these problems certainly evolve from theabuse of substances, many eventual addicts suffer from theseproblems prior to the onset of their drug use [3]. In bothcases, drug addiction has generally been treated as an acutecondition during brief episodes of residential care or severalmonths of outpatient treatment, where the primary if not
exclusive focus has been on abstinence to the exclusion ofother concerns [4]. In contrast, addiction is increasinglyregarded as a chronic relapsing disorder where recovery ispossible [5], but oen the one that requires intensive oreven multiple treatment episodes and/or strong personalor community resources. A continuing care approach isneeded to initiate and maintain recovery [6, 7]. e recov-ery movement focuses on individuals’ perceived needs andobjectives and sees abstinence as a potential resource, but notas a prerequisite, for recovery [8–10]. A recovery-orientedapproach in addiction research implies attention for theevolutions on various life domains and individuals’ subjective

2 e Scienti�c World �ournal
well being aswell as the adoption of a longitudinal perspectiveto understand the complexity of individuals’ substance usecareers and recovery processes [11].
A wide range of treatment and support services are avail-able for persons with alcohol or drug addiction problems:detox programs, drug-free outpatient treatment, methadonemaintenance therapy, long-term residential treatment pro-grams, and harm reduction services. erapeutic commu-nities (TCs) for addictions, also called drug-free or conceptTCs, aim at the reinsertion into society of former drugaddicts and were one of the �rst specialized treatment ini-tiatives for individuals with addiction problems, that evolvedoutside—and oen in reaction to—the traditional mentalhealth care. e TC history dates back to Synanon, a self-supporting community of ex-addicts founded in 1958 inSanta Monica (California) [12]. A TC can be de�ned as“a drug-free environment in which people with addictiveproblems live together in an organized and structured way topromote change toward a drug-free life in the outside society”[13]. Until the mid-1980s, TCs had a predominant positionin most Western addiction treatment systems, but due tothe drug and HIV epidemic larger scale harm reductioninitiatives (e.g., methadone maintenance, needle exchangeprograms) became the central focus of most West Europeandrug policies. Despite the long-standing and worldwideavailability of TC treatment, TCs were criticized for theirlimited coverage of drug addicts, the high costs of long-termresidential treatment, and the lack of evidence of effectivenessresulting from randomized controlled trials. Moreover, highdrop-out and relapse rates, altered client expectations andsocial norms and criticism on the impact of lengthy stays inclosed communities further questioned the appropriatenessof TC treatment around the turn of the century [14].
Although outpatient, medically-assisted (substitution)therapy is currently the most common addiction treatmentmodality [15, 16], one out of three clients in the EuropeanUnion is engaging in other types of treatment, includingtherapeutic communities [17]. Recovery-oriented treatmentin TCs starts from the widely accepted concept “communityas a method” [18] and has been implemented on all conti-nents. e standard TC model has been modi�ed to addressthe needs of speci�c populations (e.g., women with children,persons with comorbid psychiatric disorders) or new phe-nomena (e.g., TCs in prisons, methadone substitution duringTC treatment) in the so-called modi�ed TCs (MTC) [19].e TCmethod and objectives match well with the emergingrecovery movement, since TC treatment can be regardedas an educational process where individuals are supportedon their personal journey towards recovery and a drug-freelifestyle and to gain back control over their own lives [20].
Despite a long research tradition in TCs [21, 22], the evi-dence base for the effectiveness of TCs is limited according tothe prevailing Cochrane hierarchy of scienti�c evidence [23].Available reviews have been biased by a selective focus onsome types of TCs or study designs and a predominant focuson drug abstinence.e frequently cited Cochrane review bySmith and colleagues [23] only included randomized trials,while random group allocation appeared to be either notfeasible (i.e., signi�cantly higher drop-out among controls)
or advisable (i.e., motivation and self-selection are consideredto be crucial ingredients of the treatment process) in severalstudies [24, 25]. Consequently, this meta-analysis includedsome studies without true randomization and excluded alarge number of good quality quasi-experimental studies. Arecent review by Malivert and colleagues [26] le out studieson prison TCs, while this type of modi�ed TC has been themost frequently studied TC model during the last decade.Moreover, abstinence and treatment completionwere the soleoutcome measures in this study. Finally, the meta-analysis byLees and colleagues [27] can be regarded as outdated, as itdoes not include any published study since 1999.
Since sound scienti�c evidence is needed to informservice users, treatment providers, and policy makers aboutTCs’ potential to promote recovery, the aim of this paper isto review the effectiveness of TCs for addictions, based ona comprehensive systematic review of available randomizedand nonrandomized controlled studies. e paper is limitedto studies with a controlled design, as these are robuststudy designs that generate a high level of evidence. Also,nonrandomized studies were included, since the numberof randomized studies was very small (𝑛𝑛 𝑛 𝑛) and truerandomization was compromised in several studies. Giventhe focus on recovery, a range of outcome measures—apartfrom abstinence—will be evaluated and a long-term outcomeperspective will be applied, including an assessment of thein�uence of aercare or continuing support.
2. Methods
is narrative review focuses on controlled studies (random-ized trials as well as quasi-experimental designs) of thera-peutic communities for addictions. We opted for a narrativereview instead of a meta-analysis, given the heterogeneity ofthe study methodologies and the variety in data reporting.Studies were eligible if they met the following inclusioncriteria.
(i) Intervention: therapeutic communities for the treat-ment of drug addiction that are long-term hierar-chically structured (residential) educational environ-ments, where former drug users live together andwork towards recovery, and which are based on self-help and mutual help principles [12, 21].
(ii) Target population: adults addicted to illegal drugs(mostly heroin, cocaine, or amphetamines), oenin combination with an addiction to other (legal)substances (e.g., alcohol, prescription drugs). Studiesincluding persons with comorbid psychiatric disor-ders were eligible, if all study participants had a drugaddiction.
(iii) Outcome measures: at least one of the follow-ing (nonexhaustive) list of outcome measures wasreported: substance use (illicit drug use, alcohol use),length of stay in treatment (retention, treatmentcompletion/drop-out), employment status, criminalinvolvement, health and well being, family relations,quality of life, treatment status, mortality, and soforth. Objective (describing the actual situation) and

e Scienti�c World Journal 3
subjective (indicating individuals’ personal perspec-tive) indicators were considered, as well as self-report measures, biological markers, and administra-tive data.
(iv) Study design: randomized controlled trials and quasi-experimental studies that have compared prospec-tively residents that followed TC treatment with acontrol group that was treated in a usual care setting(“treatment as usual”/standard of care) or anothertype of TC (e.g., shorter program/day TC) or with acontrol group out of treatment (e.g., in prison/waitlistcontrols). Studies needed to report �ndings on TCoutcomes separately from these of other types ofinterventions (e.g., aercare).
Available reviews and meta-analyses were not included,but all studies selected for the reviews were screened basedon the aforementioned inclusion criteria. Studies that did notfocus on TC treatment, but on another type of residentialcare, were excluded from the paper. If several publicationsconcerned the same baseline sample and study design, thesepublications were regarded as one single study.
2.1. Search Strategy. We searched the following databases:ISI Web of Knowledge (WoS), PubMed, and DrugScope,up to December 31, 2011. ere were no language, coun-try, or publication year restrictions. Search strategies weredeveloped for each database, based on the search strategydeveloped for ISI Web of Knowledge, but were revisedaccordingly to take into account differences in controlledvocabulary and syntax rules. e key words we searched forwere “therapeutic communit∗” AND “drug∗ or addict∗ ordependen∗ or substance use” AND “outcome∗ or evaluationor follow-up or effectiveness.” e reference lists of retrievedstudies and of available reviews were checked for relevantstudies. In addition, the index of the International Journalof erapeutic Communities, a specialized peer-reviewedjournal on therapeutic communities and other supportiveorganisations, was screened for relevant publications.
Our search strategy revealed 997 hits, which resulted ina �rst selection of 185 records, based on title and abstract(see Figure 1). orough analysis of these abstracts bytwo independent reviewers (Mieke Autrique and WouterVanderplasschen) led to the selection of 46 studies.
In addition to the database search, conference abstracts ofEuropean Federation of erapeutic Communities (EFTC),World Federation of erapeutic Communities (WFTC),and European Working Group on Drugs Oriented Research(EWODOR) conferences and the grey literature werescanned for relevant (un)published studies.Wemade a searchof the registry of ongoing clinical trials to identify anyongoing RCTs. In case a publication could not be trackedthrough the Ghent University online library system, thestudy authors were contacted for a copy of the originalmanuscript. Finally, TC experts in various countries as wellas the European Monitoring Centre for Drugs and DrugAddiction (EMCDDA) national focal points were contactedto retrieve additional (un)published or ongoing studies thathave assessed the effectiveness of TCs for addictions.
2.2. Study Selection. In total, 46 controlled studies wereidenti�ed (28 based on the previously mentioned searchstrategy and 18 additional titles were selected based on thereference lists of selected studies and available reviews).Aer reading the full texts of these articles, 16 studies wereexcluded, because only in-treatment outcomes were reported(𝑛𝑛 𝑛 𝑛), because the treatment provided was not in line withtheTCde�nitionwe put forward (𝑛𝑛 𝑛 𝑛), or because the studydesign was deemed not a controlled design (𝑛𝑛 𝑛 𝑛). Fourstudies were excluded as they concerned secondary analysesof previously published data, usually with a focus on a speci�csubsample. Two studies did not compare TC treatment witha control intervention but rather compared outcomes relatedto speci�c client characteristics.
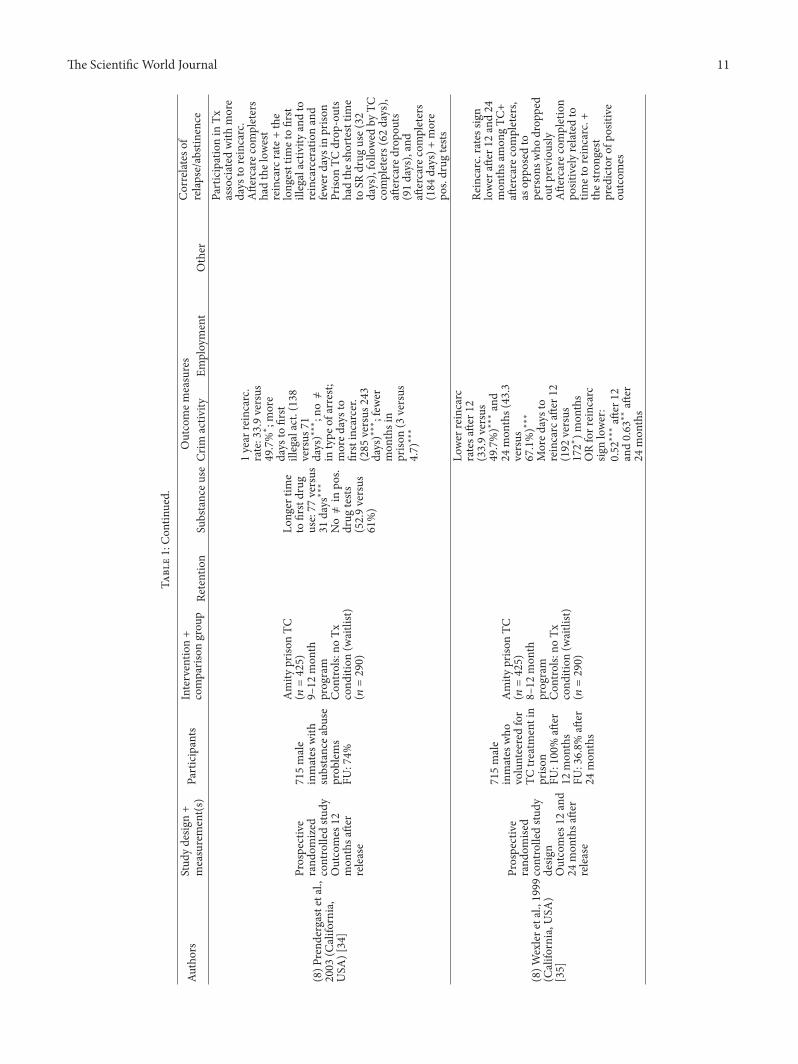
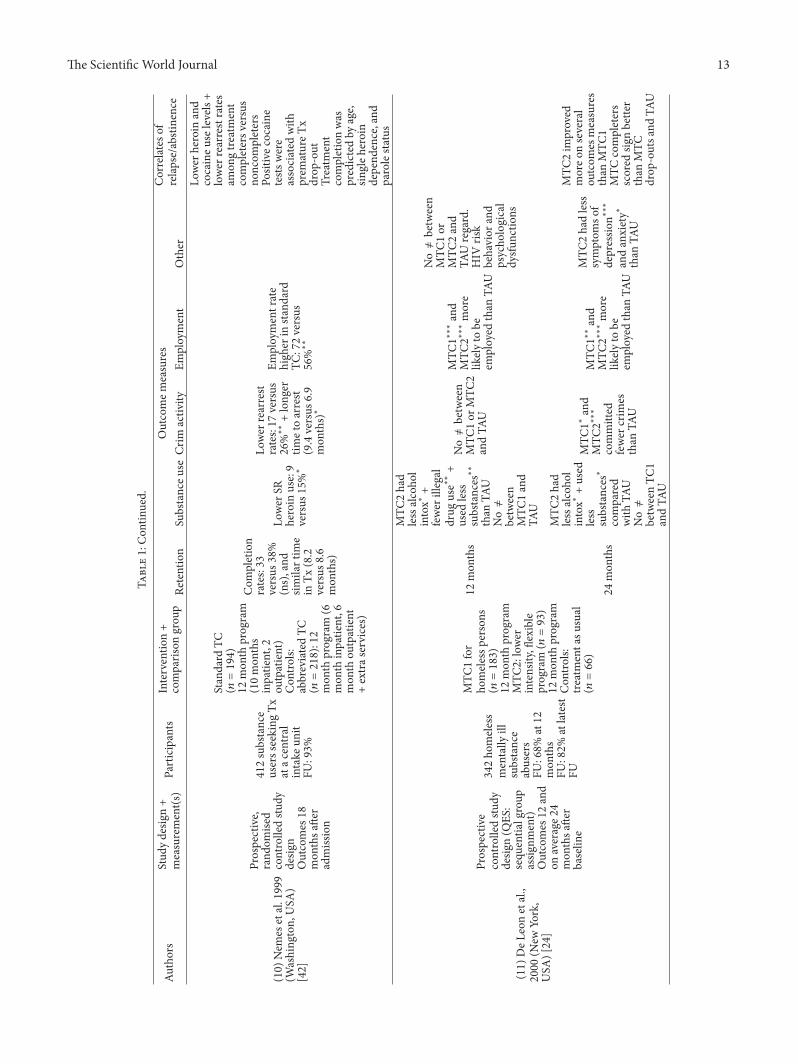
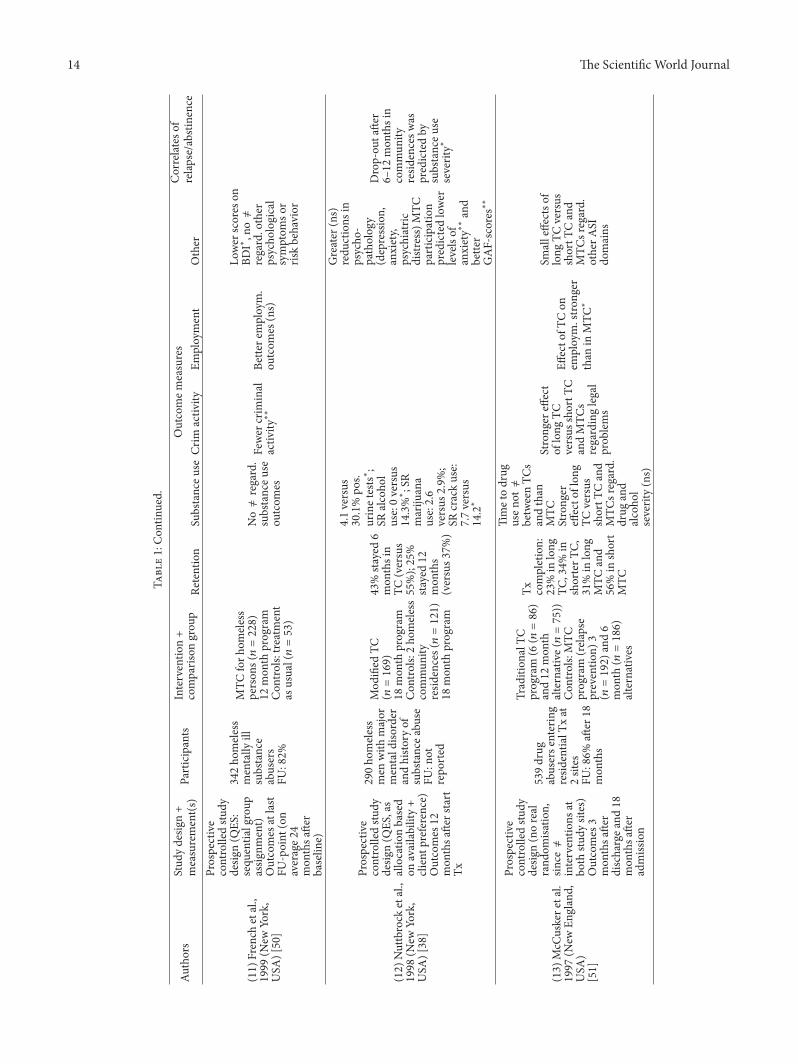
2.3. Data Extraction and Analysis. Two reviewers (MiekeAutrique and Wouter Vanderplasschen) extracted data onthe characteristics and results from the selected studies intoa large summary table (cf. Table 1). e following studycharacteristics were extracted: (1) author, country (state), andyear of publication; (2) type of study design and timing offollow-up measurements; (3) inclusion criteria and charac-teristics of the study participants + attrition rates at follow-up; (4) type of TC (including length of treatment) and typeof control condition; and (5) outcome categories: retentionand completion rates, substance use outcomes (drug andalcohol use), criminal involvement, employment, and otheroutcomes like health status, housing situation, and a columnincluding determinants/correlates of abstinence/retention.Findings from studies including multiple follow-up assess-ments were grouped and numbered accordingly (cf. Table 1).We compared reported outcomes in various categories at allreported follow-up moments post treatment (cf. Table 2.).In this summary table, “+” indicates a signi�cant differenceregarding the outcome category in favor of the experimentalcondition, while “-” indicates a signi�cant difference in favorof the control group. “�” means that no signi�cant betweengroup differences were reported; alternatively text can berephrased as follows: that no signi�cant differences werereported between the experimental and the control group.
3. Results
Based on our review of controlled studies of TC effectiveness,we identi�ed 30 publications that included a longitudinalevaluation of TCs for addictions and applied a prospectivecontrolled study design (cf. Table 1). ese 30 publicationsare based on—in total—16 original studies, since severalarticles referred to the same (large) study and/or to variousmeasurements regarding one single study (e.g., the Delawarestudy (no. 7) by Inciardi and colleagues [28–32]; the Amityprison study (no. 8) by Prendergast and colleagues [33–35]). orough methodological screening revealed that only�ve studies could be regarded as truly randomized (cf.Table 1), since in most studies the random group allocationprocess was compromised at some point [25, 36] or wasnot possible/advisable at all [24, 37, 38]. e methodologicalquality of the studies varied but was oen rather poor dueto high attrition rates, lack of objective veri�cation of study

4 e Scienti�c �orld �ournal
Records identified through database searches
WoS: 968
PubMed: 5 (add. records)
DrugScope: 24 (add. records)
Records screened based on title and abstract
WoS: 133
PubMed: 5 (add. records)
DrugScope: 16 (add. records)
Full texts assessed for eligibility
WoS: 24
PubMed: 2 (add. records)
DrugScope: 2 (add. records)
Reference lists: 18
Controlled studies
Records added based
on search of
reference lists
Records
excluded
Eligible studies Excluded studies (
Not a controlled design:
No comparison of two interventions:
Only in-treatment outcomes:
Intervention TC treatment:
Secondary analysis of previously published data:
F 1: Flowchart of the search process and number of studies retained/excluded in each phase.
�ndings, and a focus on one single study site (cf. Table 1).e oldest controlled studies date back to the beginningof the 1980s [39–41]. e bulk of studies has been carriedout/published in the 1990s. All controlled studies have beenperformed in the United States. Despite a growing researchtradition in Europe, Australia, and South America, onlyobservational uncontrolled studies have been carried out onthese continents.
e follow-up period in most controlled studies isbetween 6 and 24 months, and only three studies have fol-lowed participants for more than 36months. Study outcomesmay vary according to the follow-up moment [24, 25, 33],
but usually the magnitude of the difference(s) between theexperimental and control group diminished over time (cf.Table 2). Overall, great within-group reductions in prob-lem severity were observed between baseline and follow-up assessments, in particular regarding drug use, criminalinvolvement, and employment. e two outcome measuresthat were assessed in most studies are “substance use” and“criminal involvement.” All included studies reported at leastone outcome measure in one of both categories. Eight outof 13 (note that this number is lower than 16, as not allstudies reported outcomes concerning all categories) studiesreported at least one positive signi�cant difference between

e Scienti�c �orld �ournal 5
the TC and control group regarding legal outcomes at theone-year follow-up, while 9/14 studies found signi�cantlybetter substance use outcomes among the TC group at thattime (cf. Table 2). All studies included multiple outcomeindicators (also within one category), but only one studysucceeded to �nd several signi�cant, positive outcomesregarding most legal outcome measures (i.e., reincarcerationrate, days to �rst illegal activity/incarceration, and length ofprison sentence) [34].Most studies found only one signi�cantbetween group difference per category (e.g., time to drugrelapse), while other outcome indicators within this categorydid not differ between groups (cf. Table 1). Signi�cantlybetter outcomes in one category (e.g., substance use, criminalinvolvement) are not necessarily accompanied by improvedoutcomes on other domains (e.g., employment, psycholog-ical health). Only four studies found signi�cant differencesregarding three or more outcome categories [24, 32, 42, 43].
3.1. Treatment Retention, Health, and Social Functioning. Asopposed to all other outcome categories, TC participantsscored worse in comparison with controls on treatmentretention/completion. Only two studies showed higher reten-tion rates for the TC group, while three studies foundsigni�cantly worse completion rates among TC-participants,and six studies found non-signi�cant between group differ-ences, mostly in favor of the control condition (cf. Table 1).Substantial drop-out has been observed in most long-termTC programs, especially in the early phases of treatment [48].Studies that have compared longer and shorter TC programsusually found lower completion rates in longer and moreintensive programs [38, 51].
Five out of six studies that have reported employmentoutcomes found signi�cantly better employment rates amongTC participants. Also, �ve studies (out of 7) showed superioroutcomes on psychological symptoms, as compared withcontrols. Other outcomes that were studied are risk behavior(𝑛𝑛 𝑛 𝑛) and family and social relations (𝑛𝑛 𝑛 𝑛), which werefound to be better in two studies [32, 48].
3.2. Substance Use Outcomes. Although TC participants hadat some point posttreatment better substance use outcomesthan controls in 10 studies, substance use levels variedgreatly and overall, between 25% and 55% of the respondentsrelapsed to drug use aer 12 to 18 months. Some studiesfound very low initial relapse rates (e.g., 4% [38], 9% [42] and15% [43]), while others foundmuch higher relapse rates (e.g.,53% [34] and 69% [29]). Usually, time to relapse was longeramongTCparticipants [52].One of the few controlled studiesthat followed prison TC-participants up to three years aertheir release found a relapse rate of 77% in the TC and 94% inthe control condition [29]. Lower relapse rates were usuallyassociated with longer treatment exposure (length of stay intreatment/retention) [24, 31, 39, 41, 52] and participation insubsequent treatment or aercare [32, 35]. Treatment drop-out and relapse aer treatment were predicted in at least twostudies by the severity of substance use at baseline [28, 38].
3.3. Legal Outcomes. emajority of studies found a positiveimpact of TC treatment on diverse legal outcomes, such as
recidivism, rearrest, and reincarceration. Recidivism rates(self-reported criminal involvement) of TC participants aerone year are usually around 40%–50% [19, 31], as well asrearrest rates [29, 44], although one study reported a rearrestrate of only 17% 18 months aer the start of TC treatment[42]. Reincarceration rates 12 to 18 months aer releaseare between 30% and 55% in most studies, although Sacksand colleagues have reported clearly lower rates (19% and9%, resp.) in two studies [19, 36]. Long-term follow-upmeasurements of prison TC participants indicate rearrestrates of 63% aer three years [29] and 80% aer �ve years [44]and reincarceration rates of over 70% aer 5 years [33, 44].Again, time to reincarceration was lower in the TC groupand treatment completion and/or time in treatment predictedabsence of recidivism [28, 31, 33, 36, 42, 49]. Treatmentcompletionwas found to be associatedwith (older) age, single(instead of poly) drug dependence and being on parole [42].
3.4. Long-Term Outcomes and Outcome Predictors. Six con-trolled studies have investigated the outcomes of TC partici-pants in comparisonwith controls beyond a period of 12 to 18months (cf. Table 2). Five of these studies show signi�cantlybetter legal outcomes in favor of the TC group, while onlythree studies could demonstrate signi�cantly lower levelsof illegal drug use two years aer TC treatment. One ofthese studies [40] found a higher prevalence of alcoholproblems among TC participants at the two-year follow-up,when compared with controls who only followed a shortdetoxi�cation period.
Several studies have identi�ed correlates of relapse andrecidivism aer TC treatment. Participation in aercare[28, 35, 44], posttreatment employment [37], and older age[28, 33] were found to be the most common predictorsof abstinence and absence of rearrest (cf. Table 1). eeffectiveness of completing treatment was shown in severalstudies, as TC + aercare completers had better outcomesthan aercare drop-outs, who had in turn better outcomesthan TC completers and TC drop-outs [33, 35]. Martin andcolleagues [32] even found no differences between inmateswho followed in-prison TC treatment without subsequentaercare and controls who received usual work release.Relapse to drug use is oen associated with reoffending andreincarceration [46].
3.5. Type of Controls and TC Modalities. Eleven studies havecompared TC treatment with some form of usual care (e.g.,case management, standard treatment, and probation), and�ve studies compared one type of TC with another formof TC treatment (modi�ed versus standard TCs, or shortversus long TC programs). In the latter case, the longest/mostcomprehensive TC program was regarded as the experi-mental condition, while the shorter/least intensive programwas seen as the control condition. Only three comparisonsof longer and shorter TC programs yielded signi�cantlybetter substance use outcomes at the �rst follow-up moment[25, 41, 42], while overall few signi�cant differences wereobserved in comparison with other TC modalities. Twostudies found better employment outcomes compared withlower intensity TC models, and one study found fewer

6 �e Scienti�c �orld �ournal
T1:Overviewof
inclu
dedstu
dies
(𝑛𝑛𝑛𝑛𝑛).
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
co=m
paris
ongrou
p
Outcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
Auth
orna
mes
,ye
arof
publ
icatio
n,an
dpl
ace(
coun
try+
state)
Type
ofstu
dy(R
CT,q
uasi-
expe
rimen
tal,
etc.)
Leng
thof
follo
wup
perio
d,fo
rexa
mpl
e,ou
tcom
es12
mon
thsa
er
disc
harg
e
Num
bera
ndty
peof
partici
pant
sAt
tritio
nra
te:
how
man
yoft
heor
igin
alpa
rtici
pant
sre
triev
edat
follo
wup
?Sp
eci�
cinc
lusio
ncr
iteria
Type
ofTC
(trad
ition
al,
mod
i�ed
,pris
onTC
)+ty
peof
cont
rolc
ondi
tion
Trea
tmen
tlen
gth
Fore
xam
ple,
com
pletio
nra
tes,
mon
thsi
nTx
Fore
xam
ple,
absti
nenc
e/re
laps
erat
es%
usei
nla
stm
onth
timet
o�r
stus
eae
rTx
Fore
xam
ple,
reco
nvict
ion/
rear
rest
rates
ASIs
core
s%
rein
carc
era-
tion
Fore
xam
ple,
%em
ploy
men
t
Fore
xam
ple,
%ho
mele
ss%
psyc
hiat
ricdi
sord
ers
qual
ityof
life
fam
ilyre
latio
ns
Whi
chva
riabl
eswe
reco
rrela
ted
with
impr
oved
outco
mes
?
(1)S
acks
etal.,2012
(Colorado,USA
)[19]Pr
ospective
controlledstu
dydesig
n(partia
lrand
omisa
tion,
since
assig
nment
ratio
changed
durin
gthes
tudy)
Outcomes
12mon
thsa
er
TC-entry
127male
offenderswith
substanceu
seandmental
disordersw
hoparticipated
invario
ustypeso
fpriso
nTx
FU:86.6%
ReentryMTC
(𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
parole
supervision
case
managem
ent
(𝑛𝑛𝑛𝑛𝑛)
SRdrug
offences:37
versus
58%∗;
reincarc.rate:19
versus
38%∗
SRcrim
activ
ity:
39versus
62%∗;
days
till
reincarc.:161
versus
168∗
(2)Z
hang
etal.,
2011
(Califo
rnia,
USA
)[44]
Prospective
controlledstu
dydesig
n(Q
ES)
Outcomes
1and5
yearsa
erp
rison
release
798male
offenderswith
documented
histo
ryof
substancea
buse
FU:100%(data
from
official
records)
Priso
n-basedTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
18mon
thprogram
Con
trols:
matched
grou
pof
untre
ated
inmates
innearby
priso
n(𝑛𝑛𝑛𝑛𝑛𝑛)
1year
FU
Rearrests
:54.0
versus
47.6%
(ns);reincarc.:
54.7versus
51.9%(ns);days
inpriso
n:79.1
versus
77.4
Participationin
aercare
mediated
reincarc.rates
(ae
r1year
(ns),
notae
r5years)
andtim
einpriso
n(ae
r1∗and5
years(ns))
5year
FU
Rearrests
:80.4
versus
78.2%
(ns);reincarc:
72.4versus
72.5%(ns);days
inpriso
n:450.4
versus
412.7
(3)M
essin
aetal.,
2010
(Califo
rnia,
USA
)[45]
Prospective
rand
omise
dcontrolledstu
dydesig
nOutcomes
6and
12mon
thsa
er
release
115female
offenderswith
documented
histo
ryof
substancea
buse
FU:83%
aer
6mon
ths
FU:76%
aer
12mon
ths
Gender-respon
sive
MTC
inpriso
n(𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
stand
ard
priso
nTC
(𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Mon
thsin
aercare:2.6
versus
1.8∗
MTC
grou
phadhigh
erOR(4.60∗)
ofsuccessfu
la
ercare
completion
No≠regard.
alcoho
land
drug
ASI
compo
site
scores
+self-effi
cacy
No≠in
(time
to)returnto
custo
dy:31
versus
45%
No≠regard.
family
and
psycho
logical
ASI
compo
site
scores
Greater
redu
ction
indrug
usea
mon
gMTC
grou
p∗,
whencontrolling
forrace,em
ploy.+
marita
lstatus
Return
tocusto
dylesslik
elyam
ong
MTC
grou
p,when
controlling
for
race,employ.+
livingsta
tus

�e Scienti�c World �ournal 7
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(4)W
elsh,2007
(Pennsylvania,USA
)[37]
Prospective
controlledstu
dydesig
n(Q
ESin
5sta
tepriso
ns)
Outcomes
upto
2yearsa
errele
ase
(onaveragea
er
17mon
ths)
708male
inmates
admitted
todrug
Txin
priso
nFU
:100%
(based
onoffi
cialrecords)
5priso
nTC
s(𝑛𝑛𝑛𝑛𝑛𝑛)
Leng
thvarie
dfro
m9(𝑛𝑛𝑛𝑛)
to12
(𝑛𝑛𝑛𝑛)
and16
mon
ths(𝑛𝑛𝑛𝑛);
controls(𝑛𝑛𝑛𝑛𝑛𝑛):
3othertypes
ofdrug
Tx(drug
education,
outpatient
Tx,
self-helpgrou
ps)
No≠in
numbero
fpo
s.drug
tests
(35
versus
38%)
Lower
reincarc
andrearrest
rates,respec-
tively
30and
24%versus
41and34%∗
Reincarc.and
rearrest
respectiv
ely1.6∗
and1.5∗
times
high
eram
ong
controls
Highere
mploy.:39.2
versus
25.9%∗∗
∗
Reincarc.predicted
bypo
st-release
employmentstatus
Drugrelapse
predictedby
age
andem
ployment
(older
and
employed
person
slesslik
elyto
relapse)
(5)S
ullivan
etal.,
2007
(Colorado,
USA
)[46]
Prospective
rand
omized
controlledstu
dydesig
nOutcomes
12mon
ths
post-
release
139male
inmates
with
substanceu
seandother
psychiatric
disorders
FU:75%
(82
versus
69%)
Priso
nMTC
(𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
stand
ard
mentalh
ealth
Txin
priso
n(𝑛𝑛𝑛𝑛𝑛)
Rateso
fany
substance
use:31
versus
56%∗∗;any
illicitdrug
use:25
versus
44%∗;alcoh
olintox.:21
versus
39%∗
Timeto
relapse:3.7
versus
2.6
mon
ths∗
Sign
.associatio
nbetweenrelapse
andcommitting
new(non
drug)
offences
IncreasedORfor
reoff
ending
(4.2∗)
andreincarc.(5.8∗)
amon
gperson
swho
relapsed
insubstanceu
se
(5)S
acks
etal.,2004
(Colorado,USA
)[36]Pr
ospective
controlledstu
dydesig
n(notrue
rand
omisa
tion,
since
51subjects
moved
from
one
cond
ition
toanother)
Outcomes
12mon
thsa
er
priso
nrelease
185male
inmates
with
substanceu
seandother
psychiatric
disorders
FU:75%
(82
versus
69%)
Priso
nMTC
(𝑛𝑛𝑛𝑛𝑛)
12mon
ths
Con
trols:
stand
ard
mentalh
ealth
Tx(𝑛𝑛𝑛𝑛𝑛)
Lower
reincarc.
rates:9versus
33%∗∗;no≠
regardingother
crim
inal
outcom
es
MTC
aercare
participantshad
superio
routcomes
regardingrateso
freincarc.∗,crim
.activ
ity∗and
drug-related
crim
activ
ity∗compared
with
controls
TimeinTx
predictedabsence
ofreincarc∗∗
and
crim
activ
ity∗∗

8 �e Scienti�c World �ournal
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(6)M
orraletal.,2004
(Los
Angele
s,USA
)[47]
Prospective
controlledstu
dydesig
n(cases
assig
nedby
prob
ation)
Outcomes
12mon
thsa
erstart
TCprogram
449adolescent
prob
ationers
with
substance
abusep
roblem
sFU
:90.4%
aer
3mon
ths
FU:91.3%
aer
6mon
ths
FU:90.8%
aer
12mon
ths
MTC
inpriso
n(Pho
enix
Academ
y)(𝑛𝑛𝑛𝑛𝑛𝑛)
9mon
thprogram
Con
trols(𝑛𝑛𝑛𝑛𝑛𝑛):
alternative
prob
ation
disposition
(res.
grou
pho
mes)
No≠in
program
retention
Improved
substanceu
seou
tcom
eson
substance
prob
lem
index∗,
density
index∗,and
involvem
ent
scale∗
Greater,
nonsign.
declineso
nvario
usmeasureso
fcrim
involvem
ent
Greater
redu
ctionof
somatic∗∗
and
anxiety∗
symptom
s+sig
n.larger
redu
ctions
inpsycho
logical
symptom
sbetween3and
12mon
thFU
(7)Inciardietal.,
2004
(Delaw
are,
USA
)[28]
Prospective
controlledstu
dydesig
n(group
assig
nmentb
ycorrectio
nalstaff)
Outcomes
42and
60mon
thsa
er
baselin
e
690male
inmates
with
substancea
buse
prob
lems,
eligibleforw
ork
release
FU:69.8%
aer
48mon
ths
FU:63.8%
aer
60mon
ths
Work-release
(transitional)TC
(𝑛𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
stand
ard
workrelease,
with
outT
x(𝑛𝑛𝑛𝑛𝑛𝑛)
TC participation
stron
gest
predictoro
fdrug-fr
eesta
tusa
er4
2(O
R4.49
∗∗∗)
and60
mon
ths(OR
3.54
∗∗∗)
TCparticipation
stron
gest
predictoro
fabsenceo
frearresta
er42
(OR1.71
∗∗)a
nd60
mon
ths(OR
1.61
∗)
Older
age
predicted
drug-fr
ee∗∗
andno
rearreststa
tus∗∗∗,
whilefre
quency
ofpriord
ruguse
predictedrelapse∗
∗
aer
48mon
ths
Noprevious
Txexperie
nce
predictedrelapse
aer
60mon
ths,
whileoldera
ge∗
andbeingfemale∗
predictedno
rearrest
TCcompletion
associated
with
norearrestandbeing
drug
freea
er4
2and60
mon
ths,
with
superio
rou
tcom
esfor
person
swho
attend
edadditio
nal
aercare

�e Scienti�c World �ournal 9
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(7)M
artin
etal.,1999
(Delaw
are,USA
)[29]Pr
ospective
controlledstu
dydesig
n(partia
lrand
omization,
since
KEY
program
autom.
follo
wed
byCR
EST)
Outcomes
6,18,
and42
mon
ths
aer
baselin
e(i.e.,
1and3yearsa
er
TCperio
d)
428inmates
with
drug
abuse
prob
lems
FU:app
rox.80%
TransitionalT
C(C
REST
)(𝑛𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
priso
nTC
(KEY
)(𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Priso
nTC
+transitionalT
C(𝑛𝑛𝑛𝑛𝑛)
Regu
larw
ork
release(𝑛𝑛𝑛𝑛𝑛𝑛)
18mon
thou
tcom
es
31%
drug-fr
eeversus
16%∗
in work-release
grou
p(versus
47%in
KEY+
CRES
Tgrou
p)
57%no
trearreste
dversus
46%∗in
work-release
grou
p(versus
77%in
KEY+
CRES
Tgrou
p)
Whilegreater
expo
sure
toTC
Txledto
bette
rou
tcom
esa
er1
year,at3
yearsa
er
dischargen
o≠
werefou
ndbetweenvario
usTC
mod
alities
CRES
Tdrop
-outs
aslik
elyto
berearreste
das
work-release
grou
p,bu
tCRE
STcompleters∗∗+
CRES
T-completers
who
follo
wed
subsequent
aercare∗∗
∗were
leastlikely
tobe
arreste
dCR
ESTdrop
-outs
morelikely
tobe
drug
freethan
work-release
grou
p∗,but
CRES
Tcompleters∗∗+
CRES
T-completers
who
follo
wed
subsequent
aercare∗∗
∗even
morelikely
tobe
drug
free
42mon
thou
tcom
es
ORforb
eing
drug
free8
.2tim
eshigh
erin
CRES
T-grou
p∗∗,7.4
times
inKE
Y-grou
p∗∗,and
6.7tim
esin
KEY-CR
EST
grou
p∗compared
with
work
releaseg
roup
;23%
drug-fr
eeversus
6%∗in
work-release
grou
p
37%no
trearreste
dversus
30%in
work-release
grou
pa
er42
mon
ths
(7)L
ockw
oodetal.,
1997
(Delaw
are,
USA
)[30]
Prospective
controlledstu
dydesig
nOutcomes
6mon
ths
post-
release
483inmates
with
histo
ryof
substancea
buse
FU:app
rox.80%
TransitionalT
C(C
REST
)(𝑛𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
priso
nTC
(KEY
)(𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Priso
nTC
+transitionalT
C(𝑛𝑛𝑛𝑛𝑛)
Regu
larw
ork
release(𝑛𝑛𝑛𝑛𝑛𝑛)
87%
drug-fr
ee,
versus
71%in
KEY,73.7%
inwork
releasea
nd93.3%in
KEY-CR
EST
grou
p
86.5%no
arrest,
versus
75%in
KEY,59.9%in
workreleasea
nd97.1%in
KEY-CR
EST
grou
p

10 �e Scienti�c �orld �ournal
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(7)N
ielse
netal.,1996
(Delaw
are,USA
)[31]
Prospective
controlledstu
dydesig
n(Q
ES)
Outcomes
aer
6and18
mon
ths
689inmates
with
histo
ryof
substancea
buse
FU:77versus
72.6%a
er6
mon
ths
FU:58.5versus
36.7%a
er18
mon
ths
TransitionalT
C(C
REST
)(𝑛𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
conventio
nalw
ork
release(𝑛𝑛𝑛𝑛𝑛𝑛)
Sign
.low
errelapsea
er6
(16.2versus
62.2)∗∗∗
and
18mon
ths
(51.7versus
79%)∗∗∗
Sign
.low
errecidivism
aer
6(14.7versus
35.4)∗∗∗
and18
mon
ths(38.2
versus
63%)∗∗∗
Age,race,and
gend
erdo
not
affecto
utcomes,
butlengthof
time
inprogram
redu
cedrelapse
andrecidivism
rates(ns)
Program
completion
associated
with
fewer
relapse∗
∗∗
aer
6andfewer
recidivism
aer
6∗∗∗
and18
mon
ths∗
(7)M
artin
etal.,1995
(Delaw
are,USA
)[32]
Prospective
controlledstu
dydesig
n(Q
ES)
Outcomes
6mon
thsa
er
release
483inmates
with
histo
ryof
substancea
buse
FU:app
rox.80%
TransitionalT
C(C
REST
)(𝑛𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
priso
nTC
graduates(KE
Y)(𝑛𝑛𝑛𝑛𝑛)
Priso
nTC
+transitionalT
C(𝑛𝑛𝑛𝑛𝑛)
Regu
larw
ork
release(𝑛𝑛𝑛𝑛𝑛𝑛)
Prob
abilityof
beingdrug
freethe
high
est
amon
gCR
EST
(0.84)
∗∗∗and
KEY+
CRES
Tgrou
p(0.94)
∗∗∗
Prob.ofb
eing
arrestfre
ethe
high
estamon
gCR
EST
(0.86)
∗∗∗and
KEY+CR
EST
grou
p(0.97)
∗∗∗
Prob.ofn
olonger
injecting
theh
ighestin
CRES
T(0.97)
∗∗∗and
KEY+CR
EST
grou
p(0.97)
No≠betweenTC
onlyandwork
releaseg
roup
onanyof
theo
utcome
measures
Longer
timein
(sub
sequ
ent)Tx
theb
estp
redictor
ofdrug-fr
ee∗∗
∗and
arrest-
free∗
status
aer
Tx,asw
ellas
participationin
alonger
TCprogram
(8)P
rend
ergastetal.,
2004
(Califo
rnia,U
SA)
[33]
Prospective
rand
omized
controlledstu
dydesig
nOutcomes
5years
aer
release
715male
inmates
with
substancea
buse
prob
lems
FU:81.2%
Amity
priso
nTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
9–12
mon
thprogram
Con
trols:
noTx
cond
ition
(waitlist)
(𝑛𝑛𝑛𝑛𝑛𝑛)
Mon
ths
receivingTx
post-
release:
4.6versus
1.7∗
∗∗
Heavy
drug
usep
astyear:
24.9versus
22.6%
Reincarcerated
with
in5years:
75.7versus
83.4%∗
Daysto
reincarc:809
versus
634∗
∗∗
Stablejobin
past
year:54.8versus
52.3%
Psycho
logic.
distr
ess:31.8
versus
44.6
Reincarc.predicted
byyoun
gera
ge∗
andfewer
mon
ths
inTx
aer
release∗
∗∗
Com
pletionof
TCanda
ercare
predictedabsence
ofreincarc.∗∗
∗
�e Scienti�c World �ournal 11
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(8)P
rend
ergastetal.,
2003
(Califo
rnia,
USA
)[34]
Prospective
rand
omized
controlledstu
dyOutcomes
12mon
thsa
er
release
715male
inmates
with
substancea
buse
prob
lems
FU:74%
Amity
priso
nTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
9–12
mon
thprogram
Con
trols:
noTx
cond
ition
(waitlist)
(𝑛𝑛𝑛𝑛𝑛𝑛)
Longer
time
to�rstdrug
use:77
versus
31days
∗∗∗
No≠in
pos.
drug
tests
(52.9versus
61%)
1year
reincarc.
rate:33.9versus
49.7%∗;m
ore
days
to�rst
illegalact.(138
versus
71days)∗∗∗;no≠
intype
ofarrest;
mored
aysto
�rstincarcer.
(285
versus
243
days)∗∗∗;few
ermon
thsin
priso
n(3
versus
4.7)
∗∗∗
Participationin
Txassociated
with
more
days
toreincarc.
Ae
rcarec
ompleters
hadthelow
est
reincarc
rate+the
longesttim
eto�rst
illegalactiv
ityandto
reincarcerationand
fewer
days
inpriso
nPriso
nTC
drop
-outs
hadthes
hortesttim
eto
SRdrug
use(32
days),follo
wed
byTC
completers(62
days),
aercare
drop
outs
(91days),and
aercare
completers
(184
days)+
more
pos.drug
tests
(8)W
exlere
tal.,1999
(Califo
rnia,U
SA)
[35]
Prospective
rand
omise
dcontrolledstu
dydesig
nOutcomes
12and
24mon
thsa
er
release
715male
inmates
who
volunteeredfor
TCtre
atmentin
priso
nFU
:100%a
er12
mon
ths
FU:36.8%
aer
24mon
ths
Amity
priso
nTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
8–12
mon
thprogram
Con
trols:
noTx
cond
ition
(waitlist)
(𝑛𝑛𝑛𝑛𝑛𝑛)
Lower
reincarc
ratesa
er1
2(33.9versus
49.7%)∗∗∗
and
24mon
ths(43.3
versus
67.1%)∗∗∗
Mored
aysto
reincarc
aer
12(192
versus
172∗)m
onths
ORforreincarc
signlower:
0.52
∗∗∗a
er12
and0.63
∗∗a
er24
mon
ths
Reincarc.rates
sign
lower
aer
12and24
mon
thsa
mon
gTC
+a
ercare
completers,
asop
posedto
person
swho
drop
ped
outp
reviou
slyAe
rcarec
ompletion
positively
relatedto
timetoreincarc.+
thes
trongest
predictoro
fpositive
outcom
es

12 �e Scienti�c World �ournal
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(9)G
reenwoo
detal.,
2001
(San
Francisco,
USA
)[25]
Prospective
controlledstu
dydesig
n(only
partial
rand
omisa
tion,
since
sign.
drop
-out
amon
gcontrolbeforeT
xsta
rt)
Outcomes
6,12,
and18
mon
ths
aer
admission
261substance
abusersseeking
treatmentat
WaldenHou
seFU
:82.4%
at6
mon
ths
FU:82.7%
at12
mon
ths
FU:82.7%
at18
mon
ths
Resid
entia
lTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
dayTC
program
(sam
eTC
,but
returned
homea
tthe
endof
thed
ay)(𝑛𝑛𝑛𝑛𝑛𝑛)
Timein
program:
109.8versus
102.7days
Total
abstinence
aer
6(62.6
versus
47%),
12(47.9
versus
49%)
and18
mon
ths(50.4
versus
55.2%)
ORfor
relapsea
t6mon
ths=
3.06
∗,not
sign.
at12
and18
mon
ths
Relapsea
er1
8mon
thsp
redicted
byem
ployment
statusp
riortoTx
start∗∗
∗,injectin
gdrug
use∗
∗and
having
>1sexu
alpartner∗∗
(9)G
uydish
etal.
1999
(San
Francisco,
USA
)[48]
Prospective
controlledstu
dydesig
n(only
partial
rand
omisa
tion,
since
sign.
drop
-out
amon
gcontrolsbefore
Txsta
rt)
Outcomes
at6,
12,and
18mon
ths
188substance
abusersseeking
treatmentat
WaldenHou
sewho
participated
inall3
FU-in
terviews
Resid
entia
lTC
(𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
dayTC
program
(sam
eTC
,but
returned
homea
tthe
end
thed
ay)(𝑛𝑛𝑛𝑛𝑛)
No≠in
timeto
drop
-out
(119.7versus
108.1days)
12mon
thretentionin
dayTC
:17%
versus
9%
Lower
SCL
scores
at6∗
∗,
12∗,and
18∗
mon
ths,lower
BDIscoresa
er
12mon
ths∗,
high
ersocial
supp
ortscores
at18
mon
ths∗;
lower
social
prob
lem
severity(A
SI)∗
Mostchanges
observed
durin
g�rstmon
thso
fTx,
follo
wed
bymaintenance
ofchange
(9)G
uydish
etal.
1998
(San
Francisco,
USA
)[49]
Prospective
controlledstu
dydesig
n(only
partial
rand
omisa
tion)
Outcomes
at6
mon
ths
261substance
abusersstarting
treatmentat
WaldenHou
seFU
:82.4%
at6
mon
ths
Resid
entia
lTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
dayTC
12mon
thprogram
(𝑛𝑛𝑛𝑛𝑛𝑛)
Tx adherence
aer
6mon
ths:29
versus
34%
indayTC
;TimeinTx
:109.8versus
102.7days
Lower
ASI
severityscores
forsocial∗and
psycho
logical
prob
lems∗∗
Person
swho
stayed
>6mon
thsinTx
hadsig
nlower
legal,alcoho
l,drug
,andsocialseverity
scores
Alcoh
olseverity
redu
cedsig
n.if
person
sstayed>6
mon
thsin
resid
entia
lTC
�e Scienti�c World �ournal 13
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(10)
Nem
esetal.1999
(Washing
ton,
USA
)[42]
Prospective,
rand
omise
dcontrolledstu
dydesig
nOutcomes
18mon
thsa
er
admission
412substance
usersseeking
Txatac
entral
intake
unit
FU:93%
Standard
TC(𝑛𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
(10mon
ths
inpatie
nt,2
outpatient)
Con
trols:
abbreviatedTC
(𝑛𝑛𝑛𝑛𝑛𝑛):12
mon
thprogram
(6mon
thinpatie
nt,6
mon
thou
tpatient
+extras
ervices)
Com
pletion
rates:33
versus
38%
(ns),and
similartim
ein
Tx(8.2
versus
8.6
mon
ths)
Lower
SRheroin
use:9
versus
15%∗
Lower
rearrest
rates:17
versus
26%∗∗
+longer
timetoarrest
(9.4versus
6.9
mon
ths)∗
Employmentrate
high
erin
stand
ard
TC:72versus
56%∗∗
Lower
heroin
and
cocaineu
selevels+
lower
rearrestrates
amon
gtre
atment
completersv
ersus
noncom
pleters
Positivec
ocaine
tests
were
associated
with
prem
atureT
xdrop
-out
Treatm
ent
completionwas
predictedby
age,
singleh
eroin
depend
ence,and
parolesta
tus
(11)
DeL
eonetal.,
2000
(New
York,
USA
)[24]
Prospective
controlledstu
dydesig
n(Q
ES:
sequ
entia
lgroup
assig
nment)
Outcomes
12and
onaverage2
4mon
thsa
er
baselin
e
342ho
mele
ssmentally
illsubstance
abusers
FU:68%
at12
mon
ths
FU:82%
atlatest
FU
MTC
1for
homele
ssperson
s(𝑛𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
MTC
2:lower
intensity,�exible
program
(𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
treatmentasu
sual
(𝑛𝑛𝑛𝑛𝑛)
12mon
ths
MTC
2had
lessalcoho
lintox∗
+fewer
illegal
drug
use∗
∗+
used
less
substances
∗∗
than
TAU
No≠
between
MTC
1and
TAU
No≠between
MTC
1or
MTC
2andTA
U
MTC
1∗∗∗
and
MTC
2∗∗∗
more
likely
tobe
employed
than
TAU
No≠between
MTC
1or
MTC
2and
TAUregard.
HIV
risk
behavior
and
psycho
logical
dysfu
nctio
ns
24mon
ths
MTC
2had
lessalcoho
lintox∗
+used
less
substances
∗
compared
with
TAU
No≠
betweenTC
1andTA
U
MTC
1∗and
MTC
2∗∗∗
committed
fewer
crim
esthan
TAU
MTC
1∗∗and
MTC
2∗∗∗
more
likely
tobe
employed
than
TAU
MTC
2hadless
symptom
sof
depressio
n∗∗∗
andanxiety∗
than
TAU
MTC
2im
proved
moreo
nseveral
outcom
esmeasures
than
MTC
1MTC
completers
scored
signbette
rthan
MTC
drop
-outsa
ndTA
U
14 �e Scienti�c �orld �ournal
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(11)
French
etal.,
1999
(New
York,
USA
)[50]
Prospective
controlledstu
dydesig
n(Q
ES:
sequ
entia
lgroup
assig
nment)
Outcomes
atlast
FU-point
(on
average2
4mon
thsa
er
baselin
e)
342ho
mele
ssmentally
illsubstance
abusers
FU:82%
MTC
forh
omele
ssperson
s(𝑛𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
treatment
asusual(𝑛𝑛𝑛𝑛𝑛)
No≠regard.
substanceu
seou
tcom
esFewer
crim
inal
activ
ity∗∗
Bette
remploym.
outcom
es(ns)
Lower
scores
onBD
I∗,no≠
regard.other
psycho
logical
symptom
sor
riskbehavior
(12)
Nuttbrock
etal.,
1998
(New
York,
USA
)[38]
Prospective
controlledstu
dydesig
n(Q
ES,as
allocatio
nbased
onavailability+
clientp
reference)
Outcomes
12mon
thsa
erstart
Tx
290ho
mele
ssmen
with
major
mentald
isorder
andhisto
ryof
substancea
buse
FU:not
repo
rted
Mod
i�ed
TC(𝑛𝑛𝑛𝑛𝑛𝑛)
18mon
thprogram
Con
trols:
2ho
mele
sscommun
ityresid
ences(𝑛𝑛𝑛𝑛𝑛𝑛)
18mon
thprogram
43%sta
yed6
mon
thsin
TC(versus
55%);25%
stayed12
mon
ths
(versus3
7%)
4.1versus
30.1%po
s.urinetests∗
;SR
alcoho
luse:0versus
14.3%∗;SR
mariju
ana
use:2.6
versus
2.9%
;SR
crackuse:
7.7versus
14.2∗
Greater
(ns)
redu
ctions
inpsycho
-patholog
y(depression,
anxiety,
psychiatric
distr
ess)MTC
participation
predictedlower
levelsof
anxiety∗
∗and
bette
rGAF-scores
∗∗
Drop-ou
tae
r6–12
mon
thsin
commun
ityresid
encesw
aspredictedby
substanceu
seseverity∗
(13)
McC
uskere
tal.
1997
(New
England,
USA
)[51]
Prospective
controlledstu
dydesig
n(noreal
rand
omisa
tion,
since
≠interventio
nsat
both
study
sites)
Outcomes
3mon
thsa
er
dischargea
nd18
mon
thsa
er
admission
539drug
abuserse
ntering
resid
entia
lTxat
2sites
FU:86%
aer
18mon
ths
Tradition
alTC
program
(6(𝑛𝑛𝑛𝑛𝑛)
and12
mon
thalternative(𝑛𝑛𝑛𝑛𝑛))
Con
trols:
MTC
program
(relapse
preventio
n)3
(𝑛𝑛𝑛𝑛𝑛𝑛)
and6
mon
th(𝑛𝑛𝑛𝑛𝑛𝑛)
alternatives
Tx completion:
23%in
long
TC,34%
inshorterT
C,31%in
long
MTC
and
56%in
short
MTC
Timetodrug
usen
ot≠
betweenTC
sandthan
MTC
Stronger
effecto
flon
gTC
versus
shortT
Cand
MTC
sregard.
drug
and
alcoho
lseverity(ns)
Stronger
effect
oflong
TCversus
shortT
CandMTC
sregardinglegal
prob
lems
Effecto
fTCon
employm.stro
nger
than
inMTC
∗
Smalleffectso
flong
TCversus
shortT
Cand
MTC
sregard.
otherA
SIdo
mains

e Scienti�c �orld �ournal 15T
1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(13)
McC
uskere
tal.,
1996
(Massachusetts,
USA
)[52]
Prospective
rand
omized
controlledstu
dydesig
nOutcomes
6mon
thsa
erT
x
444drug
abuserse
ntering
oner
esidentia
lTx
facility
FU:74%
Long
MTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
6mon
thprogram
Con
trols:
short
MTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
3mon
thprogram
Program
completion:
30versus
56%in
short
TCprogram
Relapseto
drug
usein
�rstweek
aer
leaving
Tx:33versus
70%∗
Nogrou
p≠
inheroin
orcocaineu
se
Greater
improvem
entin
levelsof
depressio
nam
ongperson
ssta
ying
>80days
inTC
∗∗∗
Leng
thof
stayin
TC∗∗
+program
completion∗
pos.
associated
with
levelsof
precon
templation
Person
sstaying
>80days
inTC
had
lower
drug
use∗
∗∗
(13)
McC
uskere
tal.,
1995
(New
England,
USA
)[53]
Prospective
controlledstu
dydesig
nOutcomes
3–6
mon
thsa
er
discharge
628drug
abuserse
ntering
resid
entia
lTxat
2sites
FU:84%
inTC
versus
74%in
MTC
Tradition
alTC
program
(6(𝑛𝑛𝑛𝑛𝑛)
and12
mon
th(𝑛𝑛𝑛𝑛𝑛)a
lternative)
Con
trols:
MTC
3(𝑛𝑛𝑛𝑛𝑛𝑛)
and6
mon
thprogram
(𝑛𝑛𝑛𝑛𝑛𝑛)
40day
retention:
respectiv
ely,
70,85,73,
and72%;T
xcompletion:
respectiv
ely,
33,21,56,
30%(ns≠
in4grou
ps)
Relapse:50%
inTC
versus
44%in
MTC
No≠in
numbero
fdays
ofdrug
use
(14)
Hartm
annetal.
1997
(Miss
ouri,
USA
)[43]
Con
trolledstu
dydesig
n(Q
ES,
self-selectionfor
exp.interventio
n)Outcomes
atleast
5mon
thsa
er
release
286male
offenderswith
ahisto
ryof
substancea
buse
Noinform
ation
onFU
-rate
Priso
nTC
graduates
(𝑛𝑛𝑛𝑛𝑛𝑛)
Noinform
ationon
program
leng
thCon
trols:
comparis
ongrou
pof
eligibleperson
swho
didno
tatte
ndpriso
nTC
(𝑛𝑛𝑛𝑛𝑛𝑛)
Nosubstance
abuse:67.4
versus
62%
(ns)
Noarrest:
85.4
versus
72%∗∗
Reincarc.:16.4
versus
27.6∗
(15)
Baleetal.,1984
(Califo
rnia,U
SA)
[39]
Prospective
controlledstu
dydesig
n(only
partial
rand
omization
duetosubstantial
drop
-out
aer
grou
pallocatio
n)Outcomes
aer
2years
363male
veterans
addicted
toheroin
enterin
gwith
draw
alTx
FU:95.6%
3TC
s(𝑛𝑛𝑛𝑛𝑛𝑛):
stand
ardTC
(𝑛𝑛𝑛𝑛𝑛)+
two
MTC
s(𝑛𝑛𝑛𝑛𝑛
and
𝑛𝑛𝑛𝑛𝑛)
6mon
thprograms
Con
trols:
5-day
with
draw
alTx
(𝑛𝑛𝑛𝑛𝑛𝑛)
MeanTIP
longer
inTC
1(10.4
weeks)a
ndTC
3(11.5
weeks)∗
than
inTC
2(6.0
weeks)
Noheroin
use:40,48.1,
and35.4%
versus
33.3%
ofcontrols;
Noother
illegaldrug
use:40,41.6,
and53.3%∗
versus
39.3%
ofcontrols
Morea
lcoh
olprob
lems:40,
47.3∗∗
and
30.8%versus
22.4%of
controls
Noconvictio
n:44
∗,32.5and
59.5%∗∗
versus
31.3%of
controls
Employed/atte
nding
scho
ol:48∗,46.8and
51.9%∗∗
versus
34%
ofcontrols
Mortality:1.7%
inTC
sversus
6.6%
amon
gcontrols
e3
TCsd
iffered
largely
onprogram
characteris
tics
Heroinuse+
other
major
outcom
essig
n.bette
ramon
gsubjectssta
ying
longer
inTx

16 �e Scienti�c �orld �ournal
T1:Con
tinued.
Authors
Stud
ydesig
n+
measurement(s
)Participants
Interventio
n+
comparis
ongrou
pOutcomem
easures
Correlateso
frelapse/abstinence
Retention
Substanceu
seCr
imactiv
ityEm
ployment
Other
(15)
Baleetal.,1980
(Califo
rnia,U
SA)
[40]
Prospective
controlledstu
dydesig
n(astreated
analyses)
Outcomes
aer
1year
585male
veterans
addicted
toheroin
enterin
gwith
draw
alTx
FU:93.2%
Veterans
staying
long
(≥50
days)
(𝑛𝑛𝑛𝑛𝑛)o
rsho
rtin
TCprogram
(<50
days)(𝑛𝑛𝑛𝑛𝑛)
Con
trols:
MMT
(𝑛𝑛𝑛𝑛𝑛);detox
only(𝑛𝑛𝑛𝑛𝑛𝑛);
detox+otherT
x(𝑛𝑛𝑛𝑛𝑛𝑛)
1-year
retention
rate:<
5%in
TCversus
74.5%in
MMT
Recent
heroin
use+
anyillicit
drug
use
lower
inlong
TCsubjects
(37.3and
29.3)than
detox
only-group
(65.5and
46.9)∗∗,but
notthan
MMTgrou
p(46.6and
38.6%)
Arrest(37.3%),
convictio
n(21.3%
)and
reincarc
(4%)
ratesig
nlower
than
indetox
only-group
(54.5∗
∗,38∗
∗
and21.1%∗∗
∗,
resp.),
butn
otthan
MMT
grou
p(49.2,22,
and10.2%)
Employm./schoo
lattend
ance:65.3%
oflong
TCgrou
p,50.9%of
MMTand
38.4%∗∗
∗of
detox
only-group
Sign
.more
subjectshad
good
glob
alou
tcom
escore
inlong
TC(64%
)and
MMT(54.45%)
versus
detox
only-group
(33.8%
)
TCwith
confrontational
styleleast
successfu
lShortT
Cgrou
pdidno
tscore
sign
bette
rthandetox
only-group
Twicethe
number
oflong
TCsubjects
(29.3%
)had
the
max.global
outcom
escore
than
MMTclients
(14%
)
(29)
Coo
mbs,1981
(Califo
rnia,U
SA)
[41]
Prospective
controlledstu
dydesig
n(group
allocatio
nby
self-selection)
Outcomes
11–1
8mon
thsa
er
leavingTC
207heroin
addictsstarting
treatmentinon
eof
2TC
sFU
:78.5%
Long
-term
TC(𝑛𝑛𝑛𝑛𝑛)
12mon
thprogram
Con
trols:
short-term
TC(𝑛𝑛𝑛𝑛𝑛𝑛)
3mon
thprogram
Program
completion:
63.6versus
74.6%
Total
abstinence:
4.3versus
0%;
Return
toheroin
use:
28.6versus
53%
Program
graduates
used
lesso
enillicitdrugsa
ndwerelesslikely
tohave
relapsed
orto
berearreste
dcomparedwith
splittees.A
lsohigh
erem
ploymentrates
amon
ggraduates
TC:therapeuticcommun
ity,M
TC:m
odi�ed
therapeutic
commun
ity;SR:
self-repo
rted;�
ES:�
uasi-experim
entalstudy
;Tx:
treatment;TIP:
timein
program;B
�I:Be
ck�epressionInventory;
ASI:A
ddictio
nSeverityIndex;levelofsigni�cance:∗P<0.05;∗
∗P<0.01;∗
∗∗P<0.001.

e Scienti�c World �ournal 17
T2:Summaryof
the�
ndings
from
thes
electedstu
dies
(𝑛𝑛𝑛𝑛𝑛).
Referencen
umbero
fthe
study/studies
Type
ofTC
Com
paris
oncond
ition
Follo
wup
leng
thOutcomem
easures
Retention
Substance
use
Crim
inal
activ
ityEm
ployment
Health
Family
and
socialrelatio
ns(1)S
acks
etal.,2012
[19]
Priso
nTA
U1year
+
(2)Z
hang
etal.,2011
[44]
Priso
nTA
U1year
=5years
=(3)M
essin
aetal.,2010
[45]
Priso
nOther
TC1year
+=
==
=(4)W
elsh,2007
[37]
Priso
nTA
U2years
=+
+(5)S
ullivan
etal.,2007
[46]
Priso
nTA
U1year
++
(6)M
orraletal.,2004
[47]
Priso
nTA
U1year
=+
=+
(7)Inciardietal.,2004
[28]
Priso
nTA
U
6mon
ths
++
+1year
++
3years
+=
3years6
mon
ths
++
5years
++
(8)P
rend
ergastetal.,2004
[33]
Priso
nTA
U1year
++
2years
+5years
==
+=
=
(9)G
reenwoo
detal.,2001
[25]
Com
mun
ity-based
Other
TC6mon
ths
=+
++
1year
==
+1year
6mon
ths
=+
+(10)
Nem
esetal.,1999
[42]
Com
mun
ity-based
Other
TC1year
6mon
ths
=+
++
(11)
DeL
eonetal.,2000
[24]
Com
mun
ity-based
TAU
1year
+=
+=
2years
+=
++=
+(12)
Nuttbrock
etal.,1998
[38]
Com
mun
ity-based
TAU
1year
−+
+
(13)
McC
uskere
tal.,1997
[51]
Com
mun
ity-based
Other
TC6mon
ths
==
1year
−=
=+
(14)
Hartm
annetal.,1997
[43]
Priso
nTA
U6mon
ths
=+
(15)
Baleetal.,1984
[39]
Com
mun
ity-based
TAU
1year
−+
++
+
2years
++(illicit)
−(alcoh
ol)
++
(16)
Coo
mbs
etal.,1981
[41]
Com
mun
ity-based
Other
TC1year
=+
TC:
erapeutic
Com
mun
ity,O
ther
TC:O
ther
TCmod
ality,TAU
:TreatmentA
sUsual.

18 e Scienti�c World �ournal
psychological symptoms and relational problems among thehigher intensity treatment group. Some studies have includedmultiple control conditions [29], but usually signi�cantdifferences were only observed when the most intensiveintervention was compared with the least intensive treatmentcondition.
Most controlled studies of TC effectiveness have focusedon TCs in prison settings (𝑛𝑛 𝑛 𝑛) that prepare inmatesfor reintegration in society, while seven studies concernedTCs in the community. Whereas a substantial number ofresidents enter community TCs under legal pressure, TCtreatment in prison can be regarded as a different contextgiven the compulsory custody and conditional release termand privileges. Substance use outcomes in community TCswere signi�cantly better than those among controls in �ve(out of 6) studies, while legal outcomes were found to besuperior in three (out of 4) studies of community TCs. Onthe other hand, only in four (out of 7) studies of prison TCs,the experimental group scored signi�cantly better than thecontrol group, and only one study could demonstrate thisdifference beyond the one-year follow-up assessment [28].Six (out of 9) prison TC studies found signi�cantly betterlegal outcomes among TC participants. ree studies coulddemonstrate these gains aer two years, and two studiesfound these bene�ts maintained up to �ve years aer prisonTC treatment [28, 33].
4. Discussion
4.1. Main Findings. is narrative review was based on16 studies that have evaluated the effectiveness of TCs ascompared with other viable interventions regarding variousindicators related with recovery: substance use, criminalinvolvement, employment, psychological well being, andfamily and social relations. �ased on the study �ndings, wecan conclude that there is some evidence for the effectivenessof therapeutic community treatment. Almost two out ofthree studies have shown signi�cantly better substance useand legal outcomes at the �rst follow-up moment aertreatment among persons who stayed in a TC as comparedwith controls. Five studies found superior employment out-comes among TC participants, while another �ve studiesshowed signi�cantly fewer psychological problems in theexperimental group. Only four studies have reported signif-icantly better differential outcomes in at least three outcomecategories. is does not mean that TC participants do notimprove equally on all life domains, but these outcomes oenremained unreported or the observed progress did not differsigni�cantly from that among the control group. Severalreviews [22, 26, 27, 54] have addressed the question whetherTCs generate better outcomes than other interventions, oenleading to con�icting and not really convincing conclusions.Although several studies included in this paper showedimproved differential outcomes [28, 33, 38, 39, 42, 50], these�ndings were observed among varying populations in diversesettings, and few studies have succeeded to replicate the�ndings from other studies in exactly the same conditions.Moreover, some studies [25, 42, 45] have compared modi�edTCs with standard TCs that were not speci�cally adapted
to address the needs of special target groups. In general,such comparisons of one type of (modi�ed) TC with aless intensive (standard) TC model did not demonstratemuch between group differences, given the strong similaritiesbetween both treatment conditions. Consequently, the mainquestion is not whether one type of TC is better thananother intervention/type of TC, but rather which personsbene�t most from (what type of) TC treatment at what pointin the recovery process [22]. Also, uncontrolled treatmentoutcome studies have repeatedly shown fairly similar effectsof various types of residential treatment [55, 56] and whencompared with outpatient methadone treatment [40, 57, 58],demonstrating that—from a longitudinal perspective—nosingle intervention is superior to another. Not the differen-tial effectiveness of TCs, but rather individuals’ assets andcommunity resources and their personal needs and goals willdetermine whether TC treatment is indicated on the road torecovery.
4.2. Towards a Recovery Perspective on TC Treatment. Whilelooking beyond abstinence and desistance is warrantedfrom a recovery perspective [8], six of the selected con-trolled studies did not report other than substance use andlegal outcomes. Stable recovery in opiate addicts has beenprimarily associated with social participation and havingmeaningful activities and purposes in life, rather than withdrug abstinence or controlled drug use [59]. Focus groupswith drug users regarding their perceived quality of liferevealed few speci�c but mostly generic aspects of �o� likewell being, social inclusion, and human rights [60]. Still, apredominant focus on objective socially desirable outcomemeasures (e.g., work, alcohol and drug use, and recidivism)prevails in addiction research, whilemore subjective outcomeindicators like emotional well being, quality of life, or jobsatisfaction have largely been disregarded [61]. Such a broadperspective is also needed in TC research, as it allows amore accurate evaluation of individuals’ personal growthand well being aer TC treatment. Up to now, recoveryhas primarily been measured based on abstinence rates aerTC treatment, while abstinence is not a synonym of nor aprerequisite for recovery [8]. Total abstinence—as requiredduring and expected aer TC treatment—appears not to beself-evident, not even aer a lengthy treatment episode in aTC and subsequent continuing care. TC participants typicallyimprove on most life domains during the �rst months oftreatment and are usually able to maintain this status untilthey leave treatment [26, 48]. However, once individualsleave the TC, success rates tend to drop quickly, especiallyduring the �rst month(s) aer treatment. A recent review oflongitudinal (mostly uncontrolled) TC studies showed that21% to 100% relapsed into drug use six months to six yearsaer leaving treatment [26]. We found substantial relapserates (25%–70%) 12 to 18 months aer leaving treatment,which indicate that 30% to 75% of the studied TC sampledid not relapse within one year aer TC treatment. Althoughthe de�nition of �relapse� varied largely between studies(e.g., any substance use, illicit drug use, regular use, andlast month use), relapse can be addressed in at least twodifferent ways, depending whether one starts from an acute

e Scienti�c �orld �ournal 19
or a continuing care perspective. e former approach seesrelapse as a failure as treated individuals did not succeed toabstain from drug use aer intensive treatment. e latterperspective acknowledges the chronic relapsing nature ofdrug addiction and assumes that relapse is part and parcelof the recovery process and should rather be considered asa learning moment to keep the precarious balance betweenabstinence and relapse [62]. Factors that may contribute torecovery are longer length of stay in the TC (retention) andparticipation in subsequent aercare, since both variableshave been consistently identi�ed as predictors of improvedsubstance use outcomes [23, 26]. Surprisingly, treatmentcompletion was not found to be a predictor of abstinence,but it was associated with reduced recidivism rates in severalstudies of prison TCs [33, 36].
Treatment in TCs for addictions takes time, usuallyaround 6 to 12 months, which heightens the possibility thatresidents leave prematurely [27]. Retention in (longer term)TCs is typically lower than in shorter term programs [42, 51,55], but in general TC residents who stayed longer in treat-ment had signi�cantly better outcomes than persons whodropped out early. is has led to concerns with enhancingretention through the involvement of the family and socialnetwork and the use of senior staff [63] and with promotinginitial engagement through motivational interviewing, con-tingency management, and induction interventions [64–66].An alternative promising way of looking at retention may beto see it as the sum of treatment episodes in different servicesand the accumulation of associated treatment experiencesinstead of de�ning retention as a single uninterrupted stayin one treatment program [67]. Reentry in the communityappears to be a critical point aer TC treatment, if notprepared adequately (e.g., by providing aercare) or if drugusers go back to their old neighborhoods [68]. Some type ofcontinuing support is warranted aer TC treatment not onlyto prevent relapse, but also to link with employment/trainingand to engage in community-based activities. Moreover,treatment discharge should be dealt with in a �exible andindividualized way, since some persons will need to befurther supported or to reenter the community if they aredoing poorly.
e recovery movement starts from a longitudinal app-roach to addiction and other mental health problems [69],but few controlled studies have assessed TC outcomesbeyond a two-year follow-up period. Available studies sug-gest that—despite a fading effect of TC treatment overtime—recidivism rates continued to be signi�cantly betterthan these of controls in three studies of prison TCs [28,33, 37], while �ndings regarding substance use outcomesindicated fewer between group differences. e three-yearfollow-up outcomes of the Delaware prison study showeda 94% relapse rate among the usual care group (traditionalwork release) compared with a 77% relapse rate in the prisonaercare TC group [29]. ese �gures do not only illustratethe relapsing nature of addiction problems, but also pointat the relatively poor effectiveness of treatment programs.Although robust study designs including substantial follow-up periods that are able to retain most respondents in theanalyses are needed, one may not overestimate the lasting
effects of one single (prolonged) treatment episode. Recoveryis considered to be a lengthy process, and continuing care isneeded to maintain recovery that has been initiated during,for example, TC treatment. Some studies have shown thatthe provision of aercare was as or even more effective thaninitial TC treatment [29, 70], and the combination of TCtreatment and subsequent aercare has generated the bestresults [33, 71].
Finally, the study �ndings show that TC treatment hasgenerated bene�cial outcomes in diverse treatment settingsand may have particularly strong effects among severelyaddicted individuals like incarcerated, homeless, and men-tally ill drug addicts [22, 36, 37, 46]. erefore, treatment inTCs should be considered as a speci�c intervention, reservedfor drug addicts withmultiple and severe problems. Althoughoutpatient methadone maintenance therapy is the main-stream addiction treatment worldwide, therapeutic commu-nities for addictions can be regarded as a valuable alternativefor persons who do not do well in outpatient treatment dueto the lack of structure and supports in the community andthe fact that they live in neighborhoods that are pervasivelyaffected by drug abuse [68]. TCs can be supportive placeswhere clients can learn some of the internal control andrefusal skills conducive to stable recovery. Motivation, socialsupport and coping with stress without using substancesappear to be key factors in successful recovery [72].
4.3. Limitations of the Paper. First, most selected studies werepublished in peer reviewed journals. Although the restrictionof peer-review guarantees some form of quality control,it may have induced a selection bias as the likelihood ofretrieving non-English language articles was limited in thisway. Only results that were reported in the published paperscould be included, while it was oen unclear whether thenonreporting of some speci�c outcomes (e.g., recidivism,alcohol use) meant that this information was not collected,not analyzed, or did not yield signi�cant �ndings. Second,substantial heterogeneity has been observed between theincluded studies, not only regarding program and settingcharacteristics, but also regarding sample characteristics andoutcome measures. Despite the common “community asmethod” principle [18], TCs for addictions consist of vari-ous practices and programs with varying treatment length.Standard and modi�ed TC programs have been evaluated inthis paper, as well as TCs in prison settings and aercareTCs. is heterogeneity should be taken into account wheninterpreting the study outcomes. Although the underlyingelements may be fairly similar across TC programs, thedosage of the program and �delity to the concept mayhave varied considerably [22, 27]. Also, types of controlsvaried across studies from waitlist controls to interventionsthat differed only slightly from the experimental group(e.g., residential/longer versus day/shorter TC programs).Another limitation is the use of varying outcome measuresand instruments across studies, which further hampers thereplication and generalization of the �ndings. ird, thissystematic review was not restricted to randomized trials,although the Cochrane collaboration and other proponents

20 e Scienti�c World Journal
of the evidence-based paradigm regard this type of studydesign as the gold standard for the evaluation of evidenceof effectiveness [73]. Given the difficulties to apply thisdesign to long-term and comprehensive multi-interventionslike TCs and the low number of randomized controlledtrials on the effectiveness of TCs, a comprehensive reviewof randomized and nonrandomized controlled studies wasdeemed to be of surplus value in comparison with availablereviews, still generating an acceptable level of evidence [68].Treatment drop-outs may further compromise the validity ofthe reported results. Several studies only included substanceusers who stayed for a substantial period in the TC or whocompleted treatment but made no intent-to-treat analysis ofeveryone who started TC treatment (cf. Table 1). Finally,this is a narrative review of controlled studies that doesnot allow to weigh the �ndings from different studies or toestimate effect sizes. A meta-analysis was not possible at thispoint, given the substantial heterogeneity between programsand the diverse outcome categories and measures that werereported in the selected studies.
5. Conclusion
erapeutic communities for addictions can be regarded asrecovery-oriented programs that produce change regardingsubstance use, legal, employment, and psychological well-being outcomes among drug addicts with severe and mul-tiple problems. Despite various methodological constraints,TCs appeared to generate signi�cantly better outcomes incomparison with other viable interventions in two out ofthree studies. TC programs have usually been evaluatedfrom an acute care perspective with a primary focus onabstinence and recidivism, while a continuing care approachincludingmultiple andmore subjective outcome indicators isnecessary from a recovery perspective. If residents stay longenough in treatment and participate in subsequent aercare,TCs can play an important role on the way to recovery.Abstinencemay be just one resource to promote employmentor enhance personal well being which can in turn contributeto recovering addicts’ participation in community-basedactivities and their social inclusion.
Acknowledgments
is study was supported by the European MonitoringCentre for Drugs andDrug Addiction (EMCDDA) (Contractcode: CT.11.IBS.057). e authors would like to thank Dr.Teodora Groshkova for her support with this comprehensivereview of the outcome literature on TCs for addictions. eyare further grateful to Ilse Goethals and Mieke Autrique fortheir preparatory work for this literature review.
References
[1] R. K. Brooner, V. L. King, M. Kidorf, C. W. Schmidt Jr.,and G. E. Bigelow, “Psychiatric and substance use comorbidityamong treatment-seeking opioid abusers,” Archives of GeneralPsychiatry, vol. 54, no. 1, pp. 71–80, 1997.
[2] J. Storbjörk, e social ecology of alcohol and drug treatment[Ph.D. thesis], SoRAD, Stockholm University, Stockholm, Swe-den, 2006.
[3] R. West, eory of Addiction, Blackwell Publishing, Malden,Mass, USA, 2006.
[4] A. T. McLellan, D. C. Lewis, C. P. O’Brien, and H. D. Kleber,“Drug dependence, a chronic medical illness implications fortreatment, insurance, and outcomes evaluation,” Journal of theAmerican Medical Association, vol. 284, no. 13, pp. 1689–1695,2000.
[5] A. T. McLellan, “Have we evaluated addiction treatment cor-rectly? Implications from a chronic care perspective,”Addiction,vol. 97, no. 3, pp. 249–252, 2002.
[6] A. T. McLellan, J. R. McKay, R. Forman, J. Cacciola, and J.Kemp, “Reconsidering the evaluation of addiction treatment:from retrospective follow-up to concurrent recovery monitor-ing,” Addiction, vol. 100, no. 4, pp. 447–458, 2005.
[7] W. White, Recovery Management and Recovery-Oriented Sys-tems of Care: Scienti�c Rationale and Promising Practices, Nor-theast Addiction Technology Transfer Center, Great LakesAddiction Technology Transfer Center and PhiladelphiaDepartment of Behavioral Health & Mental RetardationServices, Pittsburgh, Pa, USA, 2008.
[8] D. Best,Addiction Recovery. AMovement For Social Change andPersonal Growth in the UK, Pavillion Publishing, Brighton, UK,2012.
[9] A. B. Laudet and W. White, “What are your priorities rightnow? Identifying service needs across recovery stages to informservice development,” Journal of Substance Abuse Treatment,vol. 38, no. 1, pp. 51–59, 2010.
[10] W. White, “Toward a new recovery advocacy movement,”in Proceedings of the Recovery Community Support ProgramConference “Working Together for Recovery”, Johnson Instituteand Faces and Voices of Recovery, Arlington, Va, USA, April2000.
[11] Y. -I. Hser andM.D. Anglin, “Addiction treatment and recoverycareers,” in Addiction Recovery Management: eory, Researchand Practice, J. F. Kelly andW. L.White, Eds., pp. 9–31, SpringerScience, New York, NY, USA, 2011.
[12] I. Goethals, V. Soyez, G. Melnick, G. D. Leon, and E. Broekaert,“Essential elements of treatment: a comparative study betweenEuropean and American therapeutic communities for addic-tion,” Substance Use and Misuse, vol. 46, no. 8, pp. 1023–1031,2011.
[13] E. Broekaert, M. Kooyman, and D. J. Ottenberg, “e “new”drug-free therapeutic community: challenging encounter ofclassic and open therapeutic communities,” Journal of SubstanceAbuse Treatment, vol. 15, no. 6, pp. 595–597, 1998.
[14] W. Vanderplasschen, S. Vandevelde, and E. Broekaert, er-apeutic Communities For Addictions in Europe. Available Evi-dence, Current Practices and Future Challenges For Recovery-Oriented Treatment in erapeutic Communities For DrugAddicts (EMCDDA Insights Publication), European MonitoringCentre for Drugs and Drug Addiction (EMCDDA), Lisbon,Portugal.
[15] P. Degkwitz and H. Zurhold, “Overview of types, charac-teristics, level of provision and utilisation of drug treatmentservices in the European member states and Norway,” inQuality of Treatment Services in Europe—Drug TreatmentSituation and Exchange of Good Practice, European Com-mission Health & Consumer Protection Directorate-General,

e Scienti�c World Journal 21
Directorate C—Public Health and Risk Assessment, Brussels,Belgium, 2008.
[16] Substance Abuse Mental Health Services Administration(SAMHSA), Alcohol and Drug Services Study (ADSS): eNational Substance Abuse Treatment System: Facilities, Clients,Services, and Staffing, Office of Applied Studies, Rockville, Md,USA, 2003.
[17] European Monitoring Centre for Drugs and Drug Addiction(EMCDDA),Annual Report on the State of the Drugs Problem inEurope 2010, European Monitoring Centre for Drugs and DrugAddiction (EMCDDA), Lisbon, Portugal, 2010.
[18] G. De Leon, Community As Method: erapeutic CommunityFor Special Populations and Special Settings, Greenwood Pub-lishing Group, Westport, Conn, USA, 1997.
[19] S. Sacks, M. Chaple, J. Y. Sacks, K. McKendrick, and M.Cleland, “Randomized trial of a re-entry modi�ed therapeuticcommunity for offenders with co-occurring disorders: crimeoutcomes,” Journal of Substance Abuse Treatment, vol. 42, no.3, pp. 247–259, 2012.
[20] G. De Leon, “Integrative recovery: a stage paradigm,” SubstanceAbuse, vol. 17, no. 1, pp. 51–63, 1996.
[21] E. Broekaert, S. Vandevelde, V. Soyez, R. Yates, and A. Slater,“e third generation of therapeutic communities: the earlydevelopment of the TC for addictions in Europe,” EuropeanAddiction Research, vol. 12, no. 1, pp. 1–11, 2006.
[22] G. De Leon, “Is the therapeutic community an evidence-basedtreatment? What the evidence says,” International Journal oferapeutic Communities, vol. 31, no. 2, pp. 104–128, 2010.
[23] L. A. Smith, S. Gates, and D. Foxcro, “erapeutic commu-nities for substance related disorder,” Cochrane Database ofSystematic Reviews, no. 1, article CD005338, 2006.
[24] G. De Leon, S. Sacks, G. Staines, and K.McKendrick, “Modi�edtherapeutic community for homeless mentally ill chemicalabusers: treatment outcomes,” American Journal of Drug andAlcohol Abuse, vol. 26, no. 3, pp. 461–480, 2000.
[25] G. L. Greenwood, W. J. Woods, J. Guydish, and E. Bein,“Relapse outcomes in a randomized trial of residential and daydrug abuse treatment,” Journal of Substance Abuse Treatment,vol. 20, no. 1, pp. 15–23, 2001.
[26] M. Malivert, M. Fatséas, C. Denis, E. Langlois, and M. Auria-combe, “Effectiveness of therapeutic communities: a systematicreview,” European Addiction Research, vol. 18, no. 1, pp. 1–11,2012.
[27] J. Lees, N. Manning, and B. Rawlings, “A culture of enquiry:research evidence and the therapeutic community,” PsychiatricQuarterly, vol. 75, no. 3, pp. 279–294, 2004.
[28] J. A. Inciardi, S. S. Martin, and C. A. Butzin, “Five-year out-comes of therapeutic community treatment of drug-involvedoffenders aer release fromprison,”Crime andDelinquency, vol.50, no. 1, pp. 88–107, 2004.
[29] S. S.Martin, C. A. Butzin, C. A. Saum, and J. A. Inciardi, “ree-year outcomes of therapeutic community treatment for drug-involved offenders in delaware: from prison to work release toaercare,” Prison Journal, vol. 79, no. 3, pp. 294–320, 1999.
[30] D. Lockwood, J. A. Inciardi, C. A. Butzin, and R. M. Hooper,“e therapeutic community continuum in corrections,” inCommunity As Method. erapeutic Communities For SpecialPopulations and Special Settings, G. De Leon, Ed., pp. 87–96,Praeger, Westport, Conn, USA, 1997.
[31] A. L. Nielsen, F. R. Scarpitti, and J. A. Inciardi, “Integratingthe therapeutic community and work release for drug-involved
offenders: the CREST program,” Journal of Substance AbuseTreatment, vol. 13, no. 4, pp. 349–358, 1996.
[32] S. S. Martin, C. A. Butzin, and J. A. Inciardi, “Assessment ofa multistage therapeutic community for drug-involved offend-ers,” Journal of Psychoactive Drugs, vol. 27, no. 1, pp. 109–116,1995.
[33] M. L. Prendergast, E. A. Hall, H. K. Wexler, G. Melnick, andY. Cao, “Amity prison-based therapeutic community: 5-Yearoutcomes,” Prison Journal, vol. 84, no. 1, pp. 36–60, 2004.
[34] M. L. Prendergast, E. A. Hall, and H. K. Wexler, “Multiple mea-sures of outcome in assessing a prison-based drug treatmentprogram,” Journal of Offender Rehabilitation, vol. 37, no. 3-4,pp. 65–94, 2003.
[35] H. K. Wexler, G. De Leon, G. omas, D. Kressel, and J. Peters,“e amity prison TC evaluation: reincarceration outcomes,”Criminal Justice and Behavior, vol. 26, no. 2, pp. 147–167, 1999.
[36] S. Sacks, J. Y. Sacks, K. McKendrick, S. Banks, and J. Stommel,“Modi�ed TC forMICAoffenders: crime outcomes,”BehavioralSciences and the Law, vol. 22, no. 4, pp. 477–501, 2004.
[37] W. N. Welsh, “A multisite evaluation of prison-based therapeu-tic community drug treatment,” Criminal Justice and Behavior,vol. 34, no. 11, pp. 1481–1498, 2007.
[38] L. A. Nuttbrock, M. Rahav, J. J. Rivera, D. S. Ng-Mak, and B. G.Link, “Outcomes of homeless mentally ill chemical abusers incommunity residences and a therapeutic community,” Psychi-atric Services, vol. 49, no. 1, pp. 68–76, 1998.
[39] R. N. Bale, V. P. Zarcone, W. W. Van Stone, J. M. Kuldau, T.M. J. Engelsing, and R. M. Elashoff, “ree therapeutic com-munities. A prospective controlled study of narcotic addictiontreatment: process and two-year follow-up results,” Archives ofGeneral Psychiatry, vol. 41, no. 2, pp. 185–191, 1984.
[40] R. N. Bale, W. W. Van Stone, J. M. Kuldau, T. M. Engelsing,R. M. Elashoff, and V. P. Zarcone, “erapeutic communitiesversus methadone maintenance: a prospective controlled studyof narcotic addiction treatment: design and one-year follow-up,” Archives of General Psychiatry, vol. 37, no. 2, pp. 179–193,1980.
[41] R. H. Coombs, “Back on the streets: therapeutic communities’impact upon drug users,”American Journal of Drug and AlcoholAbuse, vol. 8, no. 2, pp. 185–201, 1981.
[42] S. Nemes, E. D. Wish, and N. Messina, “Comparing theimpact of standard and abbreviated treatment in a therapeuticcommunity—�ndings from the district of Columbia treatmentinitiative experiment,” Journal of Substance Abuse Treatment,vol. 17, no. 4, pp. 339–347, 1999.
[43] D. J. Hartmann, J. L. Wolk, J. S. Johnston, and C. J. Colyer,“Recidivism and substance abuse outcomes in a prison-basedtherapeutic community,” Federal Probation, vol. 61, no. 4, pp.18–25, 1997.
[44] S. X. Zhang, R. E. L. Roberts, and K. E. McCollister, “erapeu-tic community in a california prison: treatment outcomes aer 5years,” Crime and Delinquency, vol. 57, no. 1, pp. 82–101, 2011.
[45] N. Messina, C. E. Grella, J. Cartier, and S. Torres, “A random-ized experimental study of gender-responsive substance abusetreatment for women in prison,” Journal of Substance AbuseTreatment, vol. 38, no. 2, pp. 97–107, 2010.
[46] C. J. Sullivan, K. McKendrick, S. Sacks, and S. Banks, “Modi�edtherapeutic community treatment for offenders with micadisorders: substance use outcomes,” American Journal of Drugand Alcohol Abuse, vol. 33, no. 6, pp. 823–832, 2007.

22 e Scienti�c World Journal
[47] A. R. Morral, D. F. McCaffrey, and G. Ridgeway, “Effec-tiveness of community-based treatment for substance-abusingadolescents: 12-Month outcomes of youths entering PhoenixAcademy or alternative probation dispositions,” Psychology ofAddictive Behaviors, vol. 18, no. 3, pp. 257–268, 2004.
[48] J. Guydish, J. L. Sorensen, M. Chan, A. Bostrom, D. Werdegar,and A. Acampora, “A randomized trial comparing day andresidential drug abuse treatment: 18-month outcomes,” Journalof Consulting andClinical Psychology, vol. 67, no. 3, pp. 428–434,1999.
[49] J. Guydish, D. Werdegar, J. L. Sorensen, W. Clark, and A. Acam-pora, “Drug abuse day treatment: a randomized clinical trialcomparing day and residential treatment programs,” Journal ofConsulting and Clinical Psychology, vol. 66, no. 2, pp. 280–289,1998.
[50] M. T. French, S. Sacks, G. De Leon, G. Staines, and K.McKendrick, “Modi�ed therapeutic community for mentallyill chemical abusers: outcomes and costs,” Evaluation and theHealth Professions, vol. 22, no. 1, pp. 60–85, 1999.
[51] J. McCusker, C. Bigelow, R. Frost et al., “e effects of plannedduration of residential drug abuse treatment on recovery andHIV risk behavior,” American Journal of Public Health, vol. 87,no. 10, pp. 1637–1644, 1997.
[52] J. Mccusker, A. Stoddard, R. Frost, and M. Zorn, “Plannedversus actual duration of drug abuse treatment: reconcilingobservational and experimental evidence,” Journal of Nervousand Mental Disease, vol. 184, no. 8, pp. 482–489, 1996.
[53] J.McCusker,M. Vickers-Lahti, A. Stoddard et al., “e effective-ness of alternative planned durations of residential drug abusetreatment,” American Journal of Public Health, vol. 85, no. 10,pp. 1426–1429, 1995.
[54] S. Sacks and J. Y. Sacks, “Research on the effectiveness ofthe modi�ed therapeutic community for persons with co-occurring substance use and mental disorders,” InternationalJournal of erapeutic Communities, vol. 31, no. 2, pp. 176–211,2010.
[55] R. H. Moos, B. S. Moos, and J. M. Andrassy, “Outcomes of fourtreatment approaches in community residential programs forpatients with substance use disorders,” Psychiatric Services, vol.50, no. 12, pp. 1577–1583, 1999.
[56] M. L. Prendergast, D. Podus, E. Chang, and D. Urada, “eeffectiveness of drug abuse treatment: a meta-analysis of com-parison group studies,” Drug and Alcohol Dependence, vol. 67,no. 1, pp. 53–72, 2002.
[57] D.D. Simpson, G.W. Joe, and B. S. Brown, “Treatment retentionand follow-up outcomes in the drug abuse treatment outcomestudy (DATOS),” Psychology of Addictive Behaviors, vol. 11, no.4, pp. 294–307, 1997.
[58] M. Gossop, J. Marsden, D. Stewart, and T. Kidd, “e NationalTreatment Outcome Research Study (NTORS): 4-5 year follow-up results,” Addiction, vol. 98, no. 3, pp. 291–303, 2003.
[59] J. De Maeyer, W. Vanderplasschen, L. Cam�eld, S. Vanheule,B. Sabbe, and E. Broekaert, “A good quality of life underthe in�uence of methadone: a qualitative study among opiate-dependent individuals,” International Journal of Nursing Studies,vol. 48, no. 10, pp. 1244–1257, 2011.
[60] J. De Maeyer, W. Vanderplasschen, and E. Broekaert,“Exploratory study on drug Users’ perspectives on qualityof life: more than health-related quality of life?” SocialIndicators Research, vol. 90, no. 1, pp. 107–126, 2009.
[61] B. Fischer, J. Rehm, G. Kim, and M. Kirst, “Eyes wide shut?—aconceptual and empirical critique of methadone maintenance
treatment,” European Addiction Research, vol. 11, no. 1, pp. 1–9,2005.
[62] W. A. Anthony, “Recovery from mental illness: the guidingvision of mental health service system in the 1990s,” Psychoso-cial Rehabilitation Journal, vol. 16, no. 4, pp. 11–23, 1993.
[63] E. Broekaert, “What future for the therapeutic community inthe �eld of addiction? A view from Europe,”Addiction, vol. 101,no. 12, pp. 1677–1678, 2006.
[64] W. N. Welsh and P. N. McGrain, “Predictors of therapeuticengagement in prison-based drug treatment,”Drug and AlcoholDependence, vol. 96, no. 3, pp. 271–280, 2008.
[65] M. L. Hiller, K. Knight, C. Leukefeld, andD. D. Simpson, “Moti-vation as a predictor of therapeutic engagement in mandatedresidential substance abuse treatment,” Criminal Justice andBehavior, vol. 29, no. 1, pp. 56–75, 2002.
[66] S. J. Bahr, A. L. Masters, and B. M. Taylor, “What works insubstance abuse treatment programs for offenders?”e PrisonJournal, vol. 92, no. 2, pp. 155–174, 2012.
[67] S. G. Mitchell, R. Morioka, H. S. Reisinger et al., “Rede�ningretention: recovery from the patients perspective,” Journal ofPsychoactive Drugs, vol. 43, no. 2, pp. 99–107, 2011.
[68] M. F. Brunette, K. T. Mueser, and R. E. Drake, “A review ofresearch on residential programs for people with severe mentalillness and co-occurring substance use disorders,” Drug andAlcohol Review, vol. 23, no. 4, pp. 471–481, 2004.
[69] C. Gagne, W. White, and W. A. Anthony, “Recovery: a commonvision for the �elds ofmental health and addictions,” PsychiatricRehabilitation Journal, vol. 31, no. 1, pp. 32–37, 2007.
[70] W. Vanderplasschen, M. Bloor, and N. McKeganey, “Long-termoutcomes of aercare participation following various forms ofdrug abuse treatment in Scotland,” Journal of Drug Issues, vol.40, no. 3, pp. 703–728, 2010.
[71] K. E. McCollister, M. T. French, M. L. Prendergast, E. Hall, andS. Sacks, “Long-term cost effectiveness of addiction treatmentfor criminal offenders: evaluating treatment history and rein-carceration �ve years post-parole,” Justice Quarterly, vol. 21, no.3, pp. 659–679, 2004.
[72] A. B. Laudet, “e road to recovery: where are we going andhow do we get there? Empirically driven conclusions and futuredirections for service development and research,” Substance Useand Misuse, vol. 43, no. 12-13, pp. 2001–2040, 2008.
[73] E. Broekaert, M. Autrique, W. Vanderplasschen, and K. Col-paert, “‘e human prerogative’: a critical analysis of evidence-based and other paradigms of care in substance abuse treat-ment,” Psychiatric Quarterly, vol. 81, no. 3, pp. 227–238, 2010.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com














