2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut

of 34
-
Upload
afdol-triatmojo-sikumbang -
Category
Documents
-
view
243 -
download
0
Transcript of 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
1/34
Abraham Ahmad A.F.
J. Nugroho
Review Article
Department of Cardiology and Vascular Medicine
Faculty of Medicine, Airlangga University - Dr.Soetomo
General Hospital
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
2/34
CLINICAL PRESENTATION AHF
Acutely
DecompensatedChronic HF
Hypertensive AHF
ACS and HF
PULMONARY EDEMA
Cardiogenic Shock
Right HF
ACS = acute coronary syndrome; HF = heart failureAdapted from Filippatos G, et al. Heart Fail Rev. 2007;12(2):87-90
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
3/34
PULMONARY EDEMA
Life-threatening
Require immediate treatment
Mortality rate : High
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
4/34
Defined as pulmonary edema due to increased capillary
hydrostatic pressure secondary to elevated pulmonary
venous pressure
McMurray JJ, 2012
Fluid accumulation with a low-protein content in the
lung interstitium and alveoli
Cardiac dysfunction
Deterioration of alveolar gas
exchange and respiratory failure
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
5/34
PATHOPHYSIOLOGY
Pathophysiologic mechanisms:
Imbalance of Starling forces - Ie, increased
pulmonary capillary pressure, decreased
plasma oncotic pressure, increased negativeinterstitial pressure
Damage to the alveolar-capillary barrier
Lymphatic obstruction Idiopathic (unknown) mechanism
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
6/34
MECHANISM OFCARDIOGENIC PULMONARY EDEMA
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
7/34
Elevated LA pressure distention and opening of
small pulmonary vesselsBlood gas exchange does not deteriorate
The progression
Fluid and colloid shift into the lung interstitium
Lymphatic outflow removes the fluid
Alveolar floodingAbnormalities in gas exchange
Vital capacity and respiratory volumes
Severe hypoxemia
Filling interstitial space (can contain up to 500mL)
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
8/34
DIAGNOSIS
History &
Physical
Examination1
Laboratory
Studies2Electrocardio
graphy3
Clinical features ofleft heart failure
Reflect evidence of
hypoxia and
increased
sympathetic tone History
to determine the
exact cause
Complete bloodcount
Electrolyte
Blood urea nitrogen
(BUN) and creatinine
Blood gas analysis
LA enlargement andLV hypertrophy
Chronic LV
dysfunction
Tachydysrhythmia or
bradydysrhythmia oracute myocardial
ischemia or
infarction
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
9/34
Brain-type
natriuretic peptide(BNP)4
High negative predictive
value
Cutoff value : 100 pg/mL BNP value of under 100
pg/mL heart failure is
unlikely
The level of BNP increase:
age, renal dysfunction
N -terminal pro BNP(NT-pro BNP)5
Well correlated with BNP
levels
NT-proBNP > 450 pg/mL(in patients 100 pg/mL
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
10/34
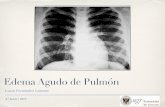
Radiography
Enlarged heart, Kerley lines, basilar edema,
pleural effusion (particularly bilateral andsymmetrical pleural effusions)
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
11/34
Echocardiography
Establish the etiology of pulmonary edema
Evaluate LV systolic and diastolic function, valvularfunction, and pericardial disease.
Non-invasive hemodynamic parameters appropriate
therapy
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
12/34
Pulmonary Arterial Catheter
Helps in differentiating CPE from Non CardiogenicPulmonary Edema (NCPE).
A PCWP exceeding 18 mm Hg indicates CPE
Monitor hemodynamic condition
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
13/34
DIFFERENTIAL DIAGNOSIS
Conditions to consider in the differentialdiagnosis of CPE include the following :
Pneumothorax
Pulmonary embolism
Respiratory failure
Acute Respiratory Distress Syndrome
Asthma
Chronic Obstructive Pulmonary Disease
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
14/34
MANAGEMENT
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
15/34
MainGoal
Reduction of
pulmonaryvenousreturn
(preload)
Reduction ofsystemicvascular
resistance(afterload)
Inotropicsupport (in
some cases)
Medical treatment
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
16/34
Vasodilators ( Nitroglycerin )
Preload reduction
Vasodilation effect lowers preloadreduce
pulmonary congestion
Should be avoided : Systolic blood pressure
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
17/34
Diuretics
Loop diuretics : Furosemide
Affect the ascending loop of Henle
Diminished renal perfusion
Delay the onset of effects of loop diuretics
Long-term use electrolyte disturbances,hypotension and worsening renal function
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
18/34
Opiates
Reduce the anxiety associated with dyspnea
Venodilators reduce preload
Reduce sympathetic drive
Depress respiratory drive
Increasing the need for invasive ventilation
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
19/34
Nesiritide
Reduce :
Left ventricular filling pressure
Pulmonary arterial pressure
Right atrial pressure
Systemic vascular resistance
Reduce levels of :
Renin, Aldosterone
Norepinephrine, and endothelin-1
Ventricular tachycardia
May cause hypotension
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
20/34
ACE inhibitor (ACEi)
Hemodynamic effects of ACEI :
Reduce afterload, improving stroke volume andcardiac output, and slightly reduce preload
improve renal perfusion diuresis
Caution in patients with :
Hypotension (systolic 3 mg / dl)
Bilateral renal artery stenosis Increased blood potassium levels (> 5 mEq / L)
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
21/34
Angiotensin II receptor blockers (ARBs)
ACEi intolerance
ACEI and ARBs Preventing remodeling,
reduce arrhythmias
The Valsartan Heart Failure (Val-HeFT) andCandesartan in Heart Failure: Assessment in
Reduction of Mortality and Morbidity(CHARM)
ARBs lowers the incidence of atrial fibrillation (AF)
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
22/34
Inotropes
When :
Reduction in preload and afterload still has not
improved
Impaired systolic function Perfusion disturbances and/or congestion
Associated with increased long-term
mortality Used only in heart failure patients with low
cardiac index and stroke volume
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
23/34
Dopamine1 Dobutamine2Norepine
phrine3
Cardiogenic shock Low dose
dopaminergic
receptors
increasing diuresis
Moderate dose
-receptors
Cardiac
contractility and
Heart rate
High dose
-receptors Vasoconstriction
(increased
afterload), Blood
pressure
Hypotension due todecreased
contractility
Positive chronotropic
& inotropic
Moderate or severe
hypotension
should be avoided
-receptorsvasoconstriction
Use in severe
hypotension
Combination with
dobutamine
improve
hemodynamic
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
24/34
Phosphodiesterase inhibitors ( milrinone )
Increase the level of intracellular cyclicadenosine monophosphate (cAMP)
Positive inotropic effect on the myocardium
Peripheral vasodilation (decreased afterload)
Reduction in pulmonary vascular resistance
(decreased preload)
Improvements in stroke volume, cardiac output,PCWP (preload), and peripheral vascular
resistance (afterload)
increased incidence of arrhythmias
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
25/34
Calcium sensitizers ( Levosimendan )
Inotropic, metabolic, and vasodilatory effects
Binding to troponin C
Not increase myocardial oxygen demand
Not a proarrhythmogenic agent
Effective and safe alternative to dobutamine
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
26/34
Ultrafiltration
Useful in patients with renal dysfunction
and diuretic resistance
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
27/34
Ultrafiltration should be considered in acute heart failure with volume overload who
do not respond to high doses of diuretics or in patients with impaired renal function
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
28/34
Intra-Aortic Balloon Pumping ( IABP )
Reducing aortic impedance and systolicpressure
In cardiogenic shock :
decreases LV filling pressures by 20-25%
improves cardiac output by 20%
Provide hemodynamic support in perioperative
and postoperative period in high-risk patients
severe coronary disease, severe LV dysfunction, orrecent MI
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
29/34
Ventilatory Support
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
30/34
Noninvasive pressure-support ventilation (NPSV)
Consider in severe CPE Two types :
CPAP and BiPAP
Improves air exchange Increases intrathoracic pressure reduction
preload & afterload
Several studies :
Decreased length of stay in the ICU
Decreased need for mechanical ventilation
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
31/34
Mechanical ventilation
When : Remain hypoxic with noninvasive supplemental
oxygenation
Impending respiratory failure
Hemodynamically unstable
Maximizes myocardial oxygen delivery and
ventilation Increase alveolar patency
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
32/34
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
33/34
Summary
Common cause of acute heart failure, life-threatening
and require immediate action
Defined as pulmonary edema due to increased capillary
hydrostatic pressure secondary to pulmonary venous
pressure
High mortality rate
Acute myocardial infarction, hypotension and a history
of frequent acute attacks increase the risk of mortality
BNP and echocardiographyImportant diagnostic tools
Therapeutic goal :
Improve the patient's symptoms
Improves fluid status
Identification of causal factors
-
8/11/2019 2.1 Dr. J. Nugroho Sp.jp - Edema Paru Akut
34/34