2014 radiation.
30
RADIATION IN PREGNANCY 2014. 3. 18. 차차차차차차차 차차차차차 차차차차 차 차 차
-
Upload
mothersafe -
Category
Health & Medicine
-
view
588 -
download
1
Transcript of 2014 radiation.

RADIATION IN PREGNANCY
2014. 3. 18.
차의과학대학교강남차병원 산부인과
조 연 경

• Ionizing Radiation IS a Teratogen!
• What is a teratogen?
• What is ionizing radiation?
• What are possible sources of ionizing radiation?
• When are the critical periods during pregnancy that ionizing radiation could affect the fetus?

• What are the levels of ionizing radiation that could affect the fetus?
• What could result if exposed to a high level of ionizing radiation during pregnancy?
• How can I protect myself from ionizing radiation poisoning?

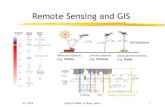
Ionizing & Non-ionizing Radiation

Commonly used measurements for ionizing radiation and their units
(Nuclear Wastelands, Makhijani et al., eds., Cambridge: MIT Press, 1995)
Units Description equivalent
Rem(roentgen equivalent man)
A unit of equivalent absorbed dose of radiation with relative biological effectiveness
rem = rad x Q
Sievert (Sv) A unit of equivalent absorbed dose equal to 100 rem.
1 Sv = 100 remSv = Gy x Q
Rad(radiation absorbed dose)
A unit of absorbed dose of radiation. Rad is a measure of the amount of energy deposited in tissue
1 rad = 100erg/gram
Gray (Gy) A unit of absorbed radiation dose equal to 100 rad. Gray is a measure of deposition of energy in tissue
1 Gy = 100 rad

Health impact of high-dose radiation from a nuclear
disaster• Cell death
– Alter DNA of normal cells
– Uncontrolled cell divisions
– Induce cancer
• Damage organs
– Acute radiation sickness (coagulopathy, immunity disorders)
– Diarrhea
– Fever, burns, coordination & equilibrium disturbances

Ionizing radiation from Natural source

Ionizing radiation from Natural source
(World Nuclear Association)

Effects of Prenatal Radiation
Exposure

Effects of radiation in pregnancy
• Pregnancy loss• Malformation• Neurobehavioral abnormalities• Fetal growth restriction --- deterministic effect --- Threshold or NOAEL (No-Adverse-Effect Level)
• Cancer --- Stochastic effect --- More radiation, greater the chance of the disease --- No defined threshold

Effects of radiation in pregnancy
- Deterministic effect
• Radiation dose, the trimester of the pregnancy
Ex) Pregnancy loss• During the 1st 2 weeks after conception, 100-200mGy
(10-20 rad)• Shortly thereafter, 250-500 mGy (25-50 rad)• 18weeks, 5000mGy (500 rad)• At term, 20, 000mGy
(2000rad)

Exposure groups Preimplantation Embryo Fetus
Spontaneous abortion
++ ± -
Congenital malformation
- + -
Intrauterine growth restriction
- + +
Mental retardation - + +
Effects of Radiation (1Gy) Prenatal Exposure in Rodents
(Schull WJ and Otake al. 1999)

Gestational age
Weeks after conception
Fetal Dose
Observed Effect
Preimplantation 0-2 5-10 radAnimal data suggest possibility of prenatal death
Major organogenesis
1-8 20-25 radAnimal and NBS data suggest that this is the most sensitive stage for growth retardation
2-15
NBS data indicate small head size; those exposed before 8 wk did not display any intellectual deficit even with small head; most sensitive time for induction of childhood cancer
Rapid neuron development and migration
8-15 >10 radSmall head size, seizures, decline in IQ points: 25points/100 rad
After organogenesis and rapid neuron development
15-term >10 radAssociated with increased frequency of childhood cancer
>50 rad Severe mental retardation observed at 16-25wk
Effects of Radiation Exposure

Ionizing radiation & CNS malformations
Malformations Estimated threshold doseGestational age at
greatest risk
Microcephaly >20Gy 8-15 week
Mental retardation
0.06-0.31Gy between 8 and 15 wks
0.25-0.28 Gy between 16 and 25 wks
>0.5Gy between 8 and 15 wks
8-15 week
Reduction of the IQ 0.1Gy 8-15 week
Other malformations (skeleton, genitals, eyes)
>0.2Gy 3-11 week

Radiation and mental retardation
• 8-15 weeks, : Risk of impaired CNS
development > 5 times than 16~25 weeks
• < 8 weeks, or > 25 weeks– No increased risk of
mental retardation

Radiation exposure & Cancer

Cancer incidence (1950-1984) and A-Bomb radiation
exposureDS86 maternal uterine dose (Gy)
0 0.01-0.29 0.30-0.59 >0.6
Mean dose (Gy) 0.000 0.087 0.416 1.372
No. at risk 710 682 129 109
Person-Years 21770 21659 4095 3287
Cancer cases 5 7 3 3
Adjusted rate per 100,000 22.4 32.5 77.8 97.0
Esstimated RR 1.00 1.24 2.18 4.78
[1.01-2.10] [1.06-6.32] 1.19-7.93

Risks of leukemia in various groups
Group Approximate risk
Increased risk over control population
occurrence
Siblings of leukemic children
1/720 4 To 10 years
Gestational exposure 1/2000 1.5 <10 years
U.S. white children <15
y.o.1/2800 1 To 10 years
(Brent RL, Teratology, 1986)

Type of riskSpontaneous risk(0 rad exposure)
Additional risk from 5 rad
Risk of very early pregnancy loss before the first missed period
350,000/106 pregnancies 0
Risk of spontaneous abortion in known pregnant women
150,000/106 pregnancies 0
Risk of major congenital malformation 30,000/106 pregnancies 0
Risk of several mental retardations 5,000/106 pregnancies 0
Risk of childhood leukemia/year 40,000/106 pregnancies/year
<?1-3/106 year
Risk of early or late-onset genetic disease 110,000/106 pregnancies Very low risk: the risk in the next generation and is not measurably increased
with small populations
Prematurity 40,000/106 pregnancies 0
Growth retardtaion 30,000/106 pregnancies 0
Stilbirth 20-2,000/106 pregnancies 0
Infertility 7% of couples 0
Spontaneous Risk Vs Additional Risk

Probability of birth with no malformation and no childhood
cancerDose to
conceptus (mGy)
No malformation
(%)
No childhood cancer(%)
No malformation
and No childhood cancer (%)
0 96.00 99.93 95.93
0.5 95.999 99.926 95.928
1.0 95.998 99.921 95.922
2.5 95.995 99.908 95.91
5.0 95.99 99.89 95.88
10.0 95.98 99.84 95.83
50.0 95.90 99.51 95.43
100.0 95.80 99.07 94.91(Wagner LK et al. 1982)

Health impact of high-dose radiation from a nuclear
disaster• ICRP (The International Commission on Radiological Protection)
– < 100mGy (10 rad)
: Not medical ground for termination
• ACOG – Threshold for medical concern ~ 50mGy (5 rad)– > 1000mGy (100 rad)
: Serious risk to fetus’ CNS---severe mental retardation– Single diagnostic radiation exposure? –10rad? 5 rad?

Estimated fetal radiation per procedure or event
Clinical suspicion Procedure Estimated fetal absorption (mGy)
Estimated fetal absorption (rad)
pnemonia X-ray chest < 0.01 <0.001
Pulmonary embolism
CT scan 0.06-0.96 0.006-0.096
Appendicitis CT scan 8-49 0.85-4.9
Nephrolithiasis Pyelogram 1.7-10 0.17-1
Breast nodule Mammogram 0.07-0.2 0.007-0.02
Colon pathology X-ray abdomen 1-4.2 0.1-0.42
Barium enema 7 0.7
Spine injury X-ray lumbar spine
6 0.6
X-ray skull <0.001 <0.001
(Groen RS et al, 2012)

Estimated fetal radiation per procedure or event
Clinical suspicion Procedure Estimated fetal absorption (mGy)
Estimated fetal absorption (rad)
Pelvic injury X-ray pelvis 1-1.4 0.11-0.4
CT scan pelvis 20-79 2.0-79
Background radiation
None 1 mSv 0.1rem
Commercial flight Round trip(toronto~frankfurt)
0.1mSv 0.01rem
100h of commercial flying
1mSv 0.1rem
(Groen RS et al, 2012)

Health impact of high-dose radiation from a nuclear
disaster• Radioactive iodine
• Fetal thyroid : extremely active from >16 weeks• Begins the uptake of iodine↑• Hypothyroidism/hyperthyroidisim• Cretinism (esp. 16-25 weeks)

It is estimated that about 3,500 new cases of cancer are diagnosed annually in pregnant women in the U.S., which is equivalent to one case every 1,000
gestations
(Pavlidis NA. Coexistence of Pregnancy and Malignancy. Oncologist 2002)
Tumor type Incidence
Breast cancer 1:3,000-10,000
Cervical cancer 1.2:10,000
Hodgkin’s disease 1:1,000-6,000
Malignant melanoma
2.6:1000
Leukemia1:75,000-100,000
Ovarian cancer1:10,000-100,000
Colorectal cancer 1:13,000
Site N %
Breast 298 26
Cervical 294 26
Leukemia 174 15
Lymphoma 119 10
Melanoma 193 8
Thyroid 45 4
Miscellaneous 111 11
Total 1,134 100

Radiotherapy during pregnancy
malignancy
No. Treatment dose(Gy,median)
Fetal dose(Gy, median)
GA at RT
No. of adverse outcomes
Brain7
40.0–54.0(42.0) 0.00270–0.08000
(0.03000)
18–28(21)
1
Breast23 30.0–78.0(41.0
0.03900–0.16000
(0.15000)
2–24(17.5)
2
Hodgkin’s lymphoma 58
6.0–44.0(36.0) 0.00100–10.00000(0.08500)
1–33(20)
3
NHL 32.0–52.0(26.0)
0.01800–0.10000
(0.06000)
4–30(23)
1
(Luis SA et al, J Med Imaging Radat Oncol 2009)

Radiotherapy during pregnancy : Cases with adverse
outcomesmalignancy Region treated Tx dose
(Gy)Fetal dose
(Gy)GA at
RTNo. of adverse
outcomes
BrainBrain
54.0 0.00270 20 Died in utero
Breast chest, axilla Perinatal death
Hodgkin’s lymphoma
Mediastinum,Supraclavicular
fossa
28 Slow learner, spontaneous
abortion
NHL Mediastinum, chest wall 26 <0.1 30
Fetal distress, short stature,
attention deficit, delayed motor development
(Luis SA et al, J Med Imaging Radiat Oncol 2009)

Radiation exposure on infants and lactating women
• Direct exposure to radiation on breast• Ingestion of radioactive pharmaceuticals
• Mammogram ---- breastfeeding (O)
• The highest radiation conc. in breast milk– 3-4 hours after adm. of radioactive pharmaceuticals– radiation absorbed by fetus < 3-10% of the total dose absorbed
by a woman– But, no negligible dose !– 1 Gy in infant :thyroid cancer(x10)
• CDC: if radioactive iodine ----stop breastfeeding !

Protection of pregnant women and fetuses from
radiation exposure• Maintaining a safe distance• Shielding one’s body from exposure• Avoiding ingestion of food and water contaminated
with radioactive particles in the air, rain, or soil
• In disaster, minimize the exposure• Lead-containing vest• In radioactive pharmaceuticals, hydration + voiding!
• If safe protocol, < 1mSv /year

Gestational age
Fetal Absorbed Dose
<5 rad 5-15 rad >15 rad
<2 wk Recommended Recommended Recommended
2-8 wk Recommended
Maybe consider termination (in presence of other severe risks)
Maybe consider termination (in presence of other risks)
8-15 wk Recommended
Maybe consider termination (in presence of other risks)
Higher risk conditions exist, but termination is not necessarily recommended
15 wk to term Recommended Recommended Recommended
Wagner LK et al : Exposure of the pregnant patient to diagnostic radiations, 1997
Continuing a pregnancy after exposure