191 Electrolyte Quiz HypoNatremia 20111117165657
5
17/11/54 1 ผู ้ป่วยหญิง แม่บ้าน อายุ 40 ปี มีการอ่อนเพลีย เวียนศีรษะมา 1 สัปดาห์ ไม่มีประวัติเจ็บป่วยมาก่อน ปฏิเสธท้องร่วง ปฏิเสธยาสมุนไพร และยาลูกกลอน BP นั่ง/ยืน 130/80 มม.ปรอท PR 70 ครั้ง/นาที , no edema Lab: Serum Osm 260 mosm/kgH 2 O Na 120, K 3.5, Cl 89, CO2 21 mEq/L Urine Osm 520 mosm/kgH 2 O, Na 50 mEq/L A. Urine diuretic B. Thyroid function test C. Serum cholesterol D. FE Na E. Serum uric acid Hyponatremia < 135 mEq/L แห้ง ปกติ บวม 1.Salt wasting Brain Tubulointerstitial 2.Extrarenal loss+ water intake 1. Hypothyroid 2. Adrenal insufficiency 3. SIADH 4. Polydipsia 1. Cirrhosis 2. CHF 3. Nephrosis High Blood sugar Low 1. Serum osmolarity High Blood sugar Low High Low Polydipsia 1. Serum osmolarity 2. Urine osmolarity
-
Upload
dokezune-aun-lookchin -
Category
Documents
-
view
23 -
download
0
Transcript of 191 Electrolyte Quiz HypoNatremia 20111117165657

17/11/54
1
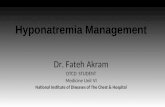
ผู้ป่วยหญิง แม่บ้าน อาย ุ40 ปี มีการอ่อนเพลีย เวียนศีรษะมา 1 สปัดาห์ ไม่มีประวตัิเจ็บป่วยมาก่อน ปฏิเสธท้องร่วง ปฏิเสธยาสมนุไพร และยาลกูกลอน BP นัง่/ยืน 130/80 มม.ปรอท PR 70 ครัง้/นาที, no edema Lab: Serum Osm 260 mosm/kgH2O Na 120, K 3.5, Cl 89, CO2 21 mEq/L Urine Osm 520 mosm/kgH2O, Na 50 mEq/L
A. Urine diuretic B. Thyroid function test C. Serum cholesterol D. FE Na E. Serum uric acid
Hyponatremia < 135 mEq/L
แหง้ ปกต ิ บวม
1.Salt wasting Brain Tubulointerstitial 2.Extrarenal loss+ water intake
1. Hypothyroid 2. Adrenal
insufficiency 3. SIADH 4. Polydipsia
1. Cirrhosis 2. CHF 3. Nephrosis
High Blood sugar
Low
1. Serum osmolarity
High Blood sugar
Low
High
Low Polydipsia
1. Serum osmolarity
2. Urine osmolarity

17/11/54
2
High Blood sugar
Low
High
Low Polydipsia
1. Serum osmolarity
2. Urine osmolarity
3. Urine Sodium
Low
High Renal loss
BP/Postural hypotension
High Blood sugar
Low
High
Low Polydipsia
4.Intravascular volume
1. Serum osmolarity
2. Urine osmolarity
3. Urine Sodium
Low
High
Normal
Renal loss
BP/Postural hypotension
High Blood sugar
Low
High
Low Polydipsia
4.Intravascular volume
1. Serum osmolarity
2. Urine osmolarity
3. Urine Sodium
Low
High
Normal
Renal loss
Salt wasting SIADH, Hypothyroid, Adrenal insufficiency
BP/Postural hypotension
Edema
High Blood sugar
Low
High
Low Polydipsia
4.Intravascular volume
1. Serum osmolarity
2. Urine osmolarity
3. Urine Sodium
Low
High
Extrarenal loss CHF/Cirrhosis/NS
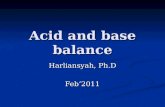
ผู้ป่วยหญิง แม่บ้าน อาย ุ40 ปี มีการอ่อนเพลีย เวียนศีรษะมา 1 สปัดาห์ ไม่มีประวตัิเจ็บป่วยมาก่อน ปฏิเสธท้องร่วง ปฏิเสธยาสมนุไพร และยาลกูกลอน 4.BP น่ัง/ยืน 130/80 มม.ปรอท PR 70 ครัง้/นาที, no edema Lab: 1.Serum Osm 260 mosm/kgH2O Na 120, K 3.5, Cl 89, CO2 21 mEq/L 2. Urine Osm 520 mosm/kgH2O, 3.Na 50 mEq/L
BP/Postural hypotension
High Blood sugar
Low
High
Low Polydipsia
4.Intravascular volume
1. Serum osmolarity
2. Urine osmolarity
3. Urine SodiumLow
High
Normal
Renal loss
Salt wasting SIADH, Hypothyroid,Adrenal insufficiency
A. Urine diuretic B. Thyroid function test C. Serum cholesterol D. FE Na E. Serum uric acid

17/11/54
3
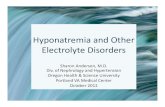
ผู้ป่วยชาย ก่อสร้าง อายุ 35 ปี มีการอ่อนเพลีย เวียนศีรษะมา 1 สปัดาห์น า้หนกัลด ไม่มีประวตัิเจ็บป่วยมาก่อน ปฏิเสธท้องร่วง ปฏิเสธยาสมนุไพรและยาลกูกลอน BP นัง่/ยืน 110/80 มม.ปรอท PR 70 ครัง้/นาที, no edema Lab: Serum Osm 260 mosm/kgH2O Na 120, K 3.5, Cl 89, CO2 22 mEq/L Urine Osm 280 mosm/kgH2O, Na 100 mEq/L
A. Water restriction 600 ml/day B. NaCl (1 g) 3x3 pc C. Furosemide 40 mg/day D. Water 600 ml plus NaCl (1 g) 3x3 pc E. 0.9% NaCl 120 ml/hr
ผู้ป่วยชาย ก่อสร้าง อายุ 35 ปี มีการอ่อนเพลีย เวียนศีรษะมา 1 สปัดาห์น า้หนกัลด ไม่มีประวตัิเจ็บป่วยมาก่อน ปฏิเสธท้องร่วง ปฏิเสธยาสมนุไพรและยาลกูกลอน 4. BP น่ัง/ยืน 110/80 มม.ปรอท PR 70 ครัง้/นาที, no edema Lab: 1. Serum Osm 260 mosm/kgH2O Na 120, K 3.5, Cl 89, CO2 22 mEq/L 2. Urine Osm 280 mosm/kgH2O, 3. Na 100 mEq/L
BP/Postural hypotension
High Blood sugar
Low
High
Low Polydipsia
4.Intravascular volume
1. Serum osmolarity
2. Urine osmolarity
3. Urine SodiumLow
High
Normal
Renal loss
Salt wasting SIADH, Hypothyroid,Adrenal insufficiency
A. Water restriction 600 ml/day B. NaCl (1 g) 3x3 pc C. Furosemide 40 mg/day D. Water 600 ml plus NaCl (1 g) 3x3 pc E. 0.9% NaCl 120 ml/hr
Clinical euvolemia Ellison DH, et al. N Engl J Med 2007;356:2064-72
Ellison DH, et al. N Engl J Med 2007;356:2064-72

17/11/54
4
ชาย อาย ุ20 ปี มีคนพบหมดสติอยูใ่นสวนสาธารณะ BP นอน 110/80 มม.ปรอท PR 80 ครัง้/นาที, ไม่มีไข้ no
edema Lab: Serum Osm 250 mosm/kgH2O Na 105, K 3.5, Cl 89, CO2 22 mEq/L Serum Cr 1.1 mg/dL Urine Osm 90 mosm/kgH2O, Na 20 mEq/L
A. Water intoxication B. SIADH C. Hypothyroidism D. Renal salt wasting nephropathy E. Cerebral salt wasting nephropathy
ชาย อาย ุ20 ปี มีคนพบหมดสติอยูใ่นสวนสาธารณะ 4.BP นอน 110/80 มม.ปรอท PR 80 ครัง้/นาที, ไม่มีไข้
no edema Lab: 1.Serum Osm 250 mosm/kgH2O Na 105, K 3.5, Cl 89, CO2 22 mEq/L Serum Cr 1.1 mg/dL 2. Urine Osm 90 mosm/kgH2O, 3.Na 20 mEq/L
High Blood sugar
Low
High
Low Polydipsia
1. Serum osmolarity
2. Urine osmolarity
A. Water intoxication B. SIADH C. Hypothyroidism D. Renal salt wasting nephropathy E. Cerebral salt wasting nephropathy
Pseudohyponatremia (Posm 280-295 mOsm/kg) -Hyperlipidemia -Hyperproteinemia
Hypertonic hyponatremia (Posm > 295 mOsm/kg) -Hyperglycemia -Mannitol
Non-osmotic ADH release (Uosm > 100 mOsm/kg)
Decreased ECF volume -Renal loss: UNa+>20 mEq/L -Extrarenal loss: UNa+< 20 mEq/L -Vomiting -Diarrhea -Excessive sweating
Normal ECF volume : UNa+>20 mEq/L -Hypothyroidism -Addison’s disease -SIADH
Increased ECF volume : UNa+<20 mEq/L -CHF -Liver failure -Nephrotic syndrome -Pregnancy
Excess water intake (Uosm < 100 mOsm/kg) -Psychogenic polydipsia -Low solute intake -Chronic kidney disease
Hypotonic hyponatremia (Posm < 275 mOsm/kg)

17/11/54
5
Ellison DH, et al. N Engl J Med 2007;356:2064-72
RANDOM HIGH
RESET OSMOLE STAT
NORMAL
HYPERSENSITIVITY
Symptomatic
Acute Duration < 48 hr
Chronic Duration >48 hr or unknown
Emergency correction needed •Hypertonic saline (3%) at 1-2 mL/kg/hr
Some immediate correction needed •Hypertonic saline (3%) at 1-2 mL/kg/hr •Perform frequent measurement of serum and urine electrolyte •Do not exceed 12 mEq/L/day
Asymptomatic
Chronic Rarely < 48 hr
No immediate correction needed
Long-term management •Identification and treatment of reversible etiologies
Reduce the ECF: retention of free water
Fluid restriction
Increased solute intake
Furosemide and Na intake
Demeclocycline
Lithium
AVP receptor antagonists
Palmer BF, et al. Nephrol Dial Transplant 15:262–268, 2000.









![fluid & electrolyte therapy 2[1].ppt FluidBasic Fluid--Electrolyte Electrolyte Disorder & Therapy ศ.พญ. สณ รตน คงเสร พงศ ภาคว ชาว สญญ](https://static.fdocument.pub/doc/165x107/5af198a37f8b9ac2468f85d0/fluid-electrolyte-therapy-21-fluidbasic-fluid-electrolyte-electrolyte-disorder.jpg)