1 Psychological Disorders Abnormal Behaviors Modules 65-69.
106
1 Psychological Disorders Abnormal Behaviors Modules 65-69
-
Upload
nathan-matthews -
Category
Documents
-
view
216 -
download
1
Transcript of 1 Psychological Disorders Abnormal Behaviors Modules 65-69.
1
Psychological Disorders
Abnormal Behaviors
Modules 65-69
2
Psychological Disorders
Perspectives on Psychological Disorders Defining Psychological Disorders
Understanding Psychological Disorders
Classifying Psychological Disorders
Labeling Psychological Disorders
3
Psychological Disorders
Anxiety Disorders Generalized Anxiety Disorder
and Panic Disorder
Phobias
Obsessive-Compulsive Disorders
Post-Traumatic Stress Disorders
Anxiety Disorder Explanation
4
Psychological Disorders
Mood Disorders Major Depressive Disorders
Bipolar Disorder
Mood Disorder Explanation
Schizophrenia Symptoms of Schizophrenia
Subtypes of Schizophrenia
5
Psychological Disorders
Schizophrenia Understanding
Schizophrenia
Personality Disorders
Rates of Psychological Disorders
6
Psychological Disorders
I felt the need to clean my room … spent four to five hour at it … At the time I loved it but then
didn't want to do it any more, but could not stop … The clothes hung … two fingers apart …I touched my bedroom wall before leaving the house … I had
constant anxiety … I thought I might be nuts.
Marc, diagnosed withobsessive-compulsive disorder
(from Summers, 1996)
7
• Whenever I get depressed it’s because I’ve lost a sense of self. I can’t find reasons to like myself. I think I’m ugly. I think no one likes me.
• Greta, diagnosed with depression (from Thorne, 1993
• Voices, like the roar of a crowd, came. I felt like Jesus; I was being crucified.
• Stuart, diagnosed with schizophrenia (from Emmons et al., 1997)
8
Psychological Disorders
People are fascinated by the exceptional, the unusual, and the abnormal. This fascination
may be caused by two reasons:
1. During various moments we feel, think, and act like an abnormal individual.
2. Psychological disorders may bring unexplained physical symptoms, irrational fears, and suicidal thoughts.
9
Psychological Disorders
To study the abnormal is the best way of understanding the normal.
1. There are 450 million people suffering from psychological disorders (WHO, 2004).
2. Depression and schizophrenia exist in all cultures of the world.
William James (1842-1910)
10
Defining Psychological Disorders
A psychological disorder is a syndrome marked by a “clinically significant disturbance in an individual’s
cognition, emotion regulation, or behavior” (American Psychiatric Association, 2013).
Disturbed, or dysfunctional, behaviors are maladaptive—they interfere with normal day-to-day
life.
Distress often accompanies dysfunctional behaviors.
Defining Psychological Disorders
11
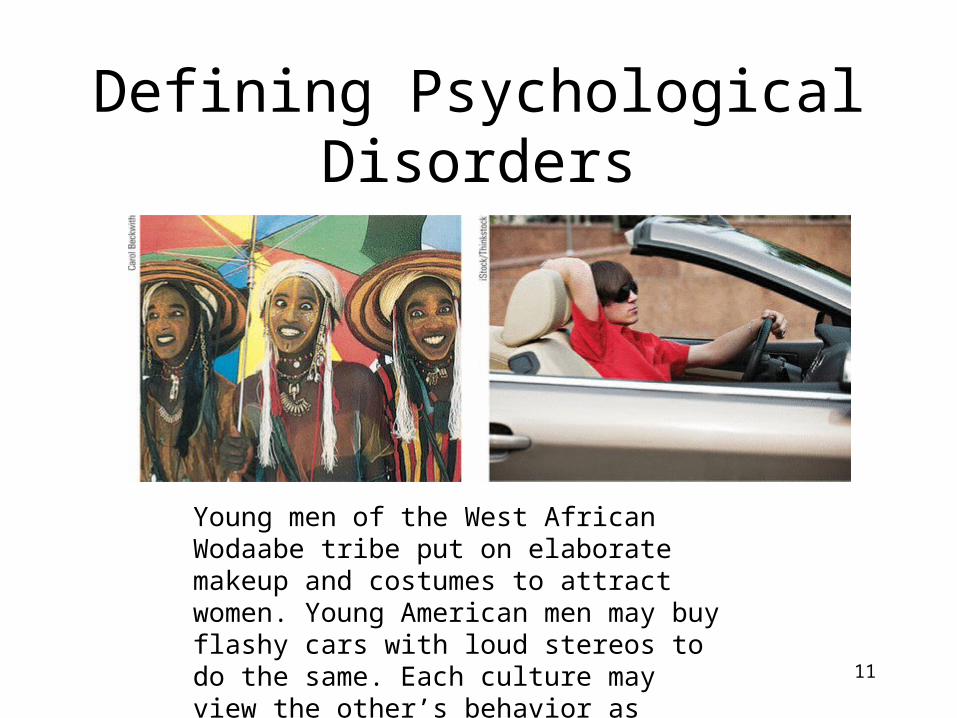
Young men of the West African Wodaabe tribe put on elaborate makeup and costumes to attract women. Young American men may buy flashy cars with loud stereos to do the same. Each culture may view the other’s behavior as abnormal.
12
Understanding Psychological Disorders
Ancient Treatments of psychological disorders include trephination, exorcism, being caged
like animals, being beaten, burned, castrated, mutilated, or transfused with animal’s blood.
Trephination (boring holes in the skull to remove evil forces)
John W. V
erano
13
Medical Perspective
Philippe Pinel (1745-1826) from France, insisted that madness was not due to demonic
possession, but an ailment of the mind.
Dance in the madhouse.
George W
esley Bellow
s, Dancer in a M
adhouse, 1907. © 1997 T
he Art Institute of C
hicago
Mental illness- is also called psychopathology
14
Medical Model• The concept that diseases or psychological
disorders have physical causes that can be diagnosed, treated, and in most cases, cured, often through treatment in a hospital.
Mental illness is also called psychopathology.
15
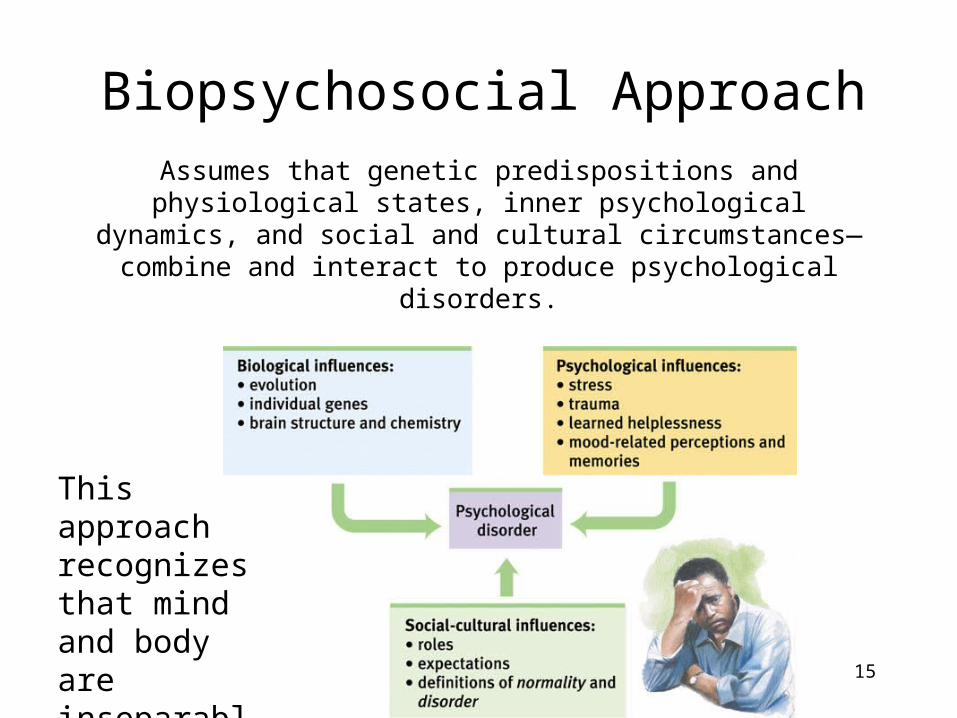
Biopsychosocial ApproachAssumes that genetic predispositions and
physiological states, inner psychological dynamics, and social and cultural circumstances— combine and
interact to produce psychological disorders.
This approach recognizes that mind and body are inseparable.
Classifying Psychological Disorders
• In psychiatry and psychology, diagnostic classification aims not only to describe a disorder but also to predict its future course, imply appropriate treatment, and stimulate research into its causes.
• The most common system for describing disorders and estimating how often they occur is the American Psychiatric Association’s 2013 Diagnostic and Statistical Manual of Mental Disorders, now in its fifth edition (DSM-5).
The New DSM-5
• Some diagnostics labels have changed.– Ex. “Autism” and “Asperger’s syndrome”
are no longer included; they have been combined into “autism spectrum disorder”
– Ex. “Mental retardation” has become “intellectual disability.”
– Ex. New categories include “hoarding disorder” and “binge-eating disorder.”
17
An Example of a Diagnosis• A person may be diagnosed with and treated for “insomnia
disorder” if he or she meets all of the following criteria:• Is dissatisfied with sleep quantity or quality (difficulty
initiating, maintaining, or returning to sleep).• Sleep disturbance causes distress or impairment in
everyday functioning.• Occurs at least three nights per week.• Present for at least three months.• Occurs despite adequate opportunity for sleep.• Is not explained by another sleep disorder (such as
narcolepsy).• Is not caused by substance use or abuse.• Is not caused by other mental disorders or medical
conditions
18
19
Goals of DSM
1. Describe (400) disorders.2. Determine how prevalent the
disorder is.
Disorders outlined by DSM-V are reliable. Therefore, diagnoses by different professionals are similar.Critics have long faulted the DSM for casting too wide a net and bringing “almost any kind of behavior within the compass of psychiatry” (Eysenck et al., 1983). They worry that the DSM-5 will extend the pathologizing of everyday life—for example, by turning bereavement grief into depression and boyish rambunctiousness into ADHD (Frances, 2013).
Labeling Psychological Disorders
1. Critics of the DSM-IV argue that labels may stigmatize individuals.
Once we label a person, we view that person differently (Farina, 1982). Labels create preconceptions that guide our perceptions and our interpretations.
20
Asylum baseball team (labeling)
21
Labeling Psychological Disorders
2. Labels may be helpful for healthcare professionals when communicating with one another and establishing therapy.
22
Labeling Psychological Disorders
3. “Insanity” labels raise moral and ethical questions about how society should treat people who have disorders and have committed crimes.
Theodore Kaczynski(Unabomber)
Elaine T
hompson/ A
P Photo
Rates of Psychological Disorders
Rates of Psychological Disorders
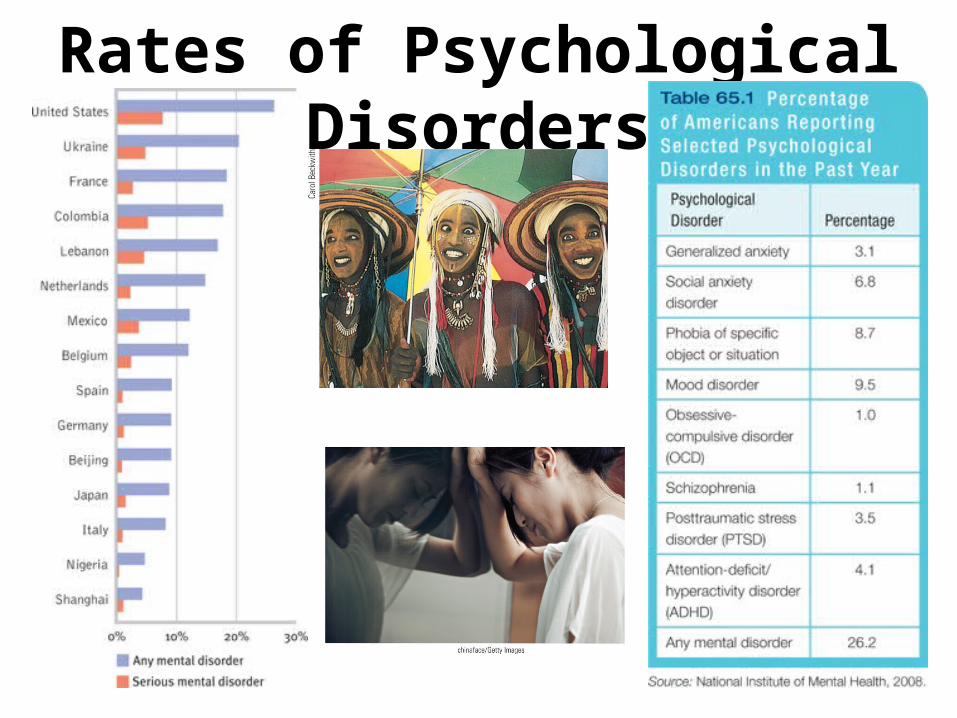
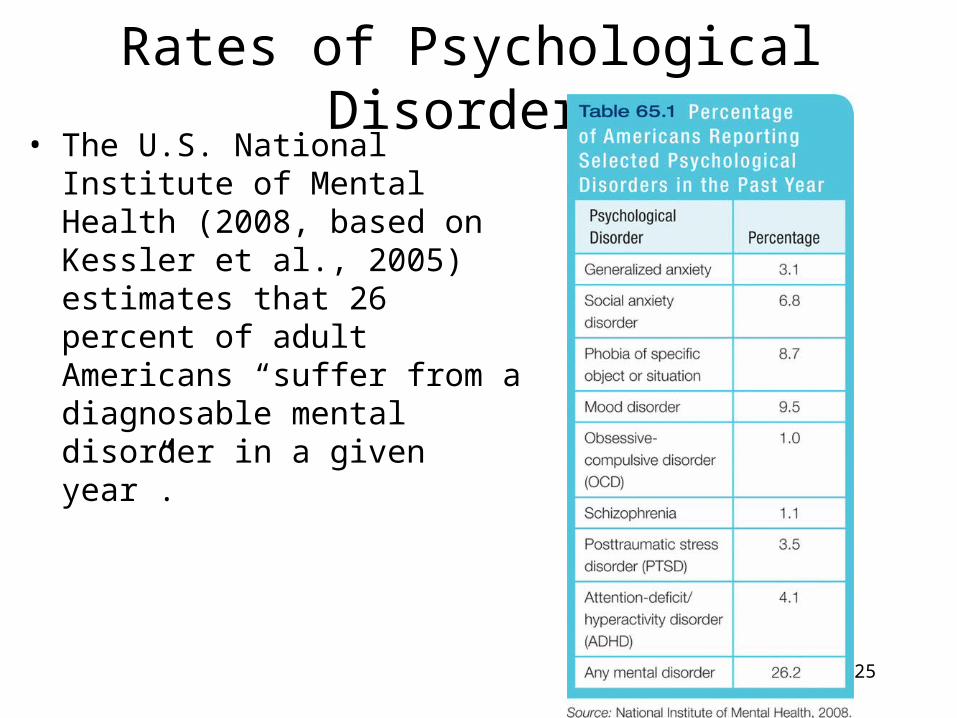
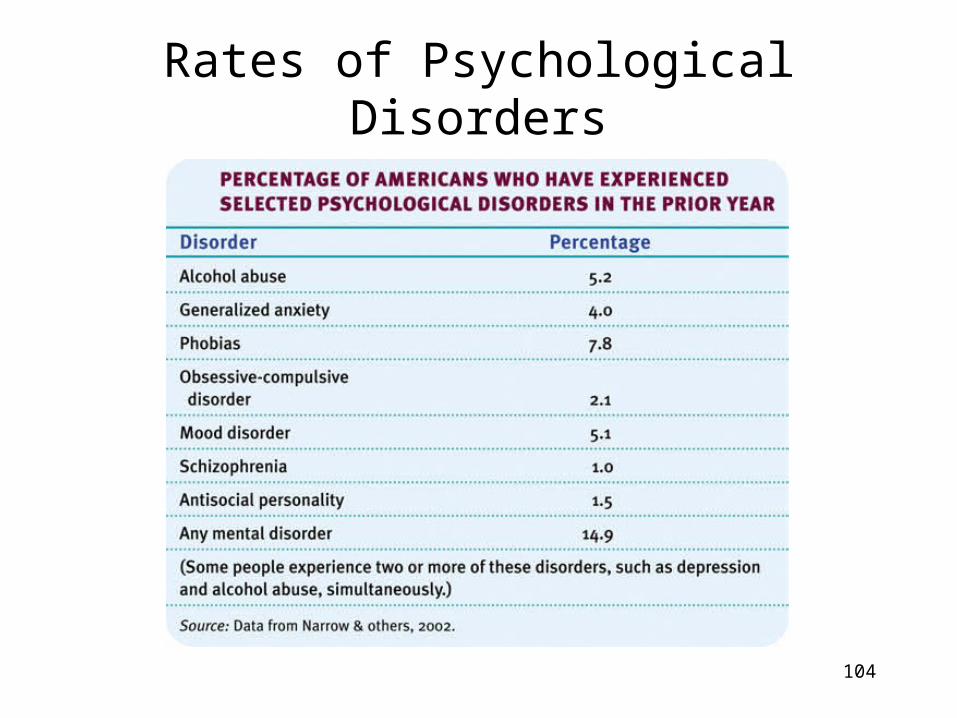
• The U.S. National Institute of Mental Health (2008, based on Kessler et al., 2005) estimates that 26 percent of adult Americans “suffer from a diagnosable mental disorder in a given year”.
25
Who is most vulnerable to mental disorders?
• The incidence of serious psychological disorders has been doubly high among those below the poverty line (CDC, 1992).
• Does poverty cause disorders? Or do disorders cause poverty? It is both, though the answer varies with the disorder. Schizophrenia understandably leads to poverty. Yet the stresses and demoralization of poverty can also precipitate disorders, especially depression in women and substance use disorder in men (Dohrenwend et al., 1992).
26
27
Anxiety Disorders
Feelings of excessive apprehension and anxiety.
1. Generalized anxiety disorders
2. Phobias3. Panic disorders
3Types
28
Generalized Anxiety Disorder
1. Persistent and uncontrollable tenseness and apprehension.
2. Autonomic arousal.3. Inability to identify or avoid the cause of certain feelings.4. Constantly worried bad things might happen.5. Plagued by muscular tension, agitation and sleeplessness.
Symptoms
Generalized Anxiety Disorder
• One of generalized anxiety disorder’s worst characteristics is that the person may not be able to identify, and therefore deal with or avoid, its cause. To use Sigmund Freud’s term, the anxiety is free-floating.
• Many people with generalized anxiety disorder were maltreated and inhibited as children (Moffitt et al., 2007a). As time passes, however, emotions tend to mellow, and by age 50, generalized anxiety disorder becomes fairly rare (Rubio & López-Ibor, 2007).
29
Generalized Anxiety Disorder
• Treatments– Psychotherapy with or
without drugs– The most frequently
prescribed are tranquilizers that belong to the group known as benzodiazepines: diazepam, and alprazolam
30
31
Panic Disorder
• Entails an anxiety tornado. Panic strikes suddenly, wreaks havoc, and disappears.
• Minute-long episodes of intense dread which may include feelings of terror, chest pains, choking, or other frightening sensations.– Heart palpitations and shortness of breath is
sometimes mistaken for a heart attack.• Anxiety is a component of both disorders. It
occurs more in the panic disorder, making people avoid situations that cause it.
Panic Disorder
• Treatments
– Usually with drugs belonging to the group of benzodiazepines, antidepressants (Prozac-reuptake inhibitors), and psychotherapy.
32
33
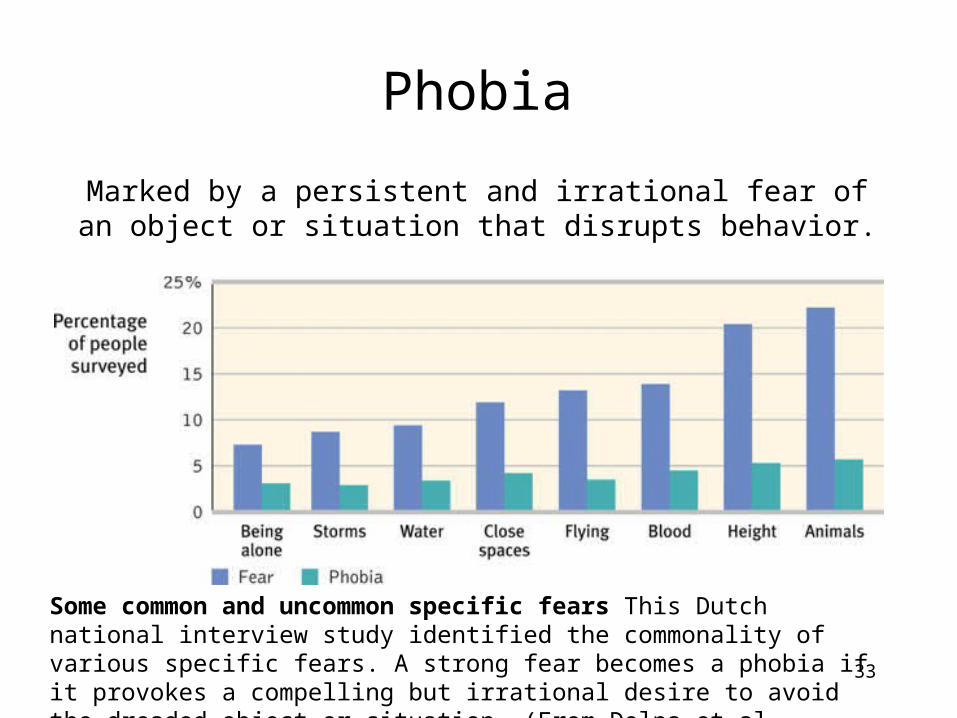
Phobia
Marked by a persistent and irrational fear of an object or situation that disrupts behavior.
Some common and uncommon specific fears This Dutch national interview study identified the commonality of various specific fears. A strong fear becomes a phobia if it provokes a compelling but irrational desire to avoid the dreaded object or situation. (From Delpa et al., 2008.)
Phobias
• Social anxiety disorder (formerly called social phobia) is shyness taken to an extreme. – an intense fear of being scrutinized
by others– avoid potentially embarrassing social
situations– eating out, or going to parties—or will
sweat or tremble when doing so
34
35
Kinds of Phobias
Phobia of blood.Hemophobia
Phobia of closed spaces.
Claustrophobia
Phobia of heights.Acrophobia
Phobia of open places.Agoraphobia
Social Phobia of performing in social situations.
36
Obsessive-Compulsive Disorder• Persistence of unwanted thoughts (obsessions)
and urges to engage in senseless rituals (compulsions) that cause distress.
• Obsessive thoughts and compulsive behaviors cross the fine line between normality and disorder when they persistently interfere with everyday living and cause distress.– Checking to see if the door is locked is OK– Checking the door 10 times is NOT.– Washing your hands over and over until they are raw is
NOT OK.• OCD is more common among teens and young adults
than among older people (Samuels & Nestadt, 1997).
Obsessive-Compulsive Disorder

Obsessive-Compulsive Disorder
• Treatments– Exposure therapy
– Antidepressant drugs
38
39
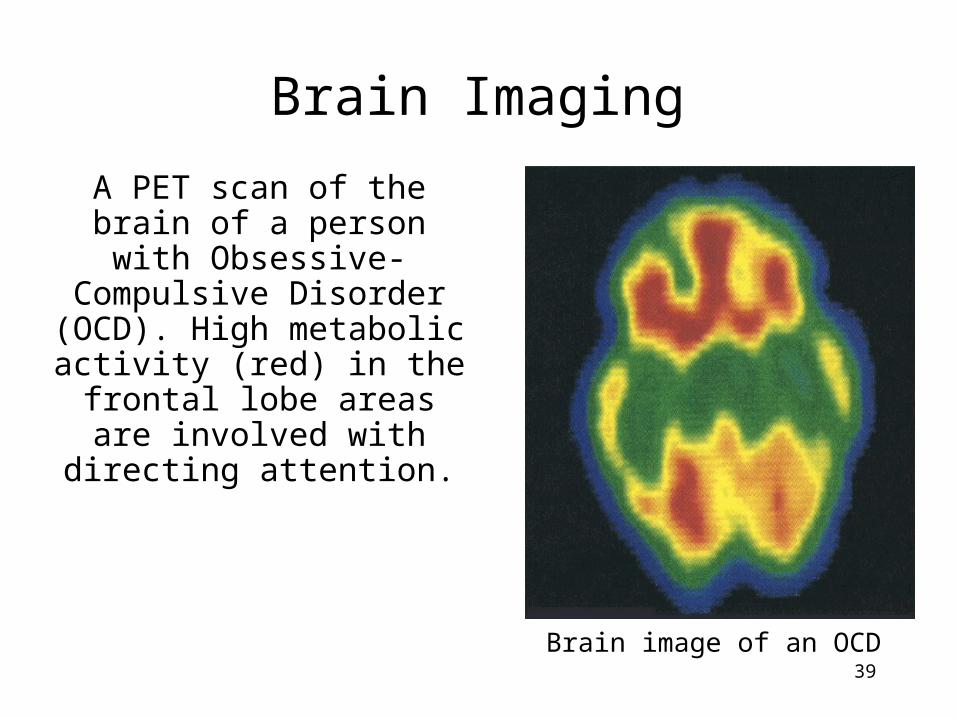
A PET scan of the brain of a person with Obsessive-Compulsive Disorder (OCD). High
metabolic activity (red) in the frontal
lobe areas are involved with
directing attention.
Brain Imaging
Brain image of an OCD
40
Post-Traumatic Stress Disorder
Four or more weeks of the following symptoms constitute post-traumatic
stress disorder (PTSD):
1. Haunting memories
2. Nightmares3. Social withdrawal
4. Jumpy anxiety
5. Sleep problems
Bettm
ann/ Corbis
Post-Traumatic Stress Disorder
• Is not just do to a war situation.• PTSD symptoms have also been reported by
survivors of accidents, disasters, and violent and sexual assaults (including an estimated two-thirds of prostitutes).
• Some psychologists believe that PTSD has been overdiagnosed, due partly to a broadening definition of trauma (Dobbs, 2009; McNally, 2003).
41
Resilience to PTSD• Only about 1 in 10 women and 1 in 20 of men
react to traumatic situations and develop PTSD. • More than 9 in 10 New Yorkers, although stunned
and grief-stricken by 9/11, did not respond pathologically.
• All major religions of the world suggest that surviving a trauma leads to the growth of an individual.
• Indeed, suffering can lead to “benefit finding”-post-traumatic growth: positive psychological changes as a result of struggling with extremely challenging circumstances and life crises.
42
43
Explaining Anxiety Disorders
• Freud’s psychoanalytic theory proposed that, beginning in childhood, people repress intolerable impulses, ideas, and feelings and that this submerged mental energy sometimes produces mystifying symptoms, such as anxiety.
• Today’s psychologists have instead turned to two contemporary perspectives—learning and biological.
44
The Learning Perspective•Learning theorists suggest that fear conditioning leads to anxiety.
– Classical conditioning– Fear dogs because once
bitten; accidents.•This anxiety then becomes associated with other objects or events (stimulus generalization) and is reinforced.
– When a person fears heights after a fall and later develops a fear of flying.
John Coletti/ Stock, B
oston
The Learning Perspective: Observational Learning
• Investigators believe that fear responses are inculcated through observational learning.
• Young monkeys develop fear when they watch other monkeys who are afraid of snakes.
• Humans likewise learn fears by observing others (Olsson et al., 2007).
45
Cognition• Our interpretations and irrational
beliefs can also cause feelings of anxiety.
• People with anxiety disorder also tend to be hypervigilant. – A pounding heart becomes a sign of a
heart attack. – A lone spider near the bed becomes a
likely infestation.46
The Biological Perspective• Natural Selection:• We humans seem biologically prepared to
fear threats faced by our ancestors. • Our phobias focus on such specific fears:
spiders, snakes, and other animals; enclosed spaces and heights; storms and darkness.
• Therefore, fear preserves the species.• Twin studies suggest that our genes may be
partly responsible for developing fears and anxiety. Twins are more likely to share phobias.
47
.
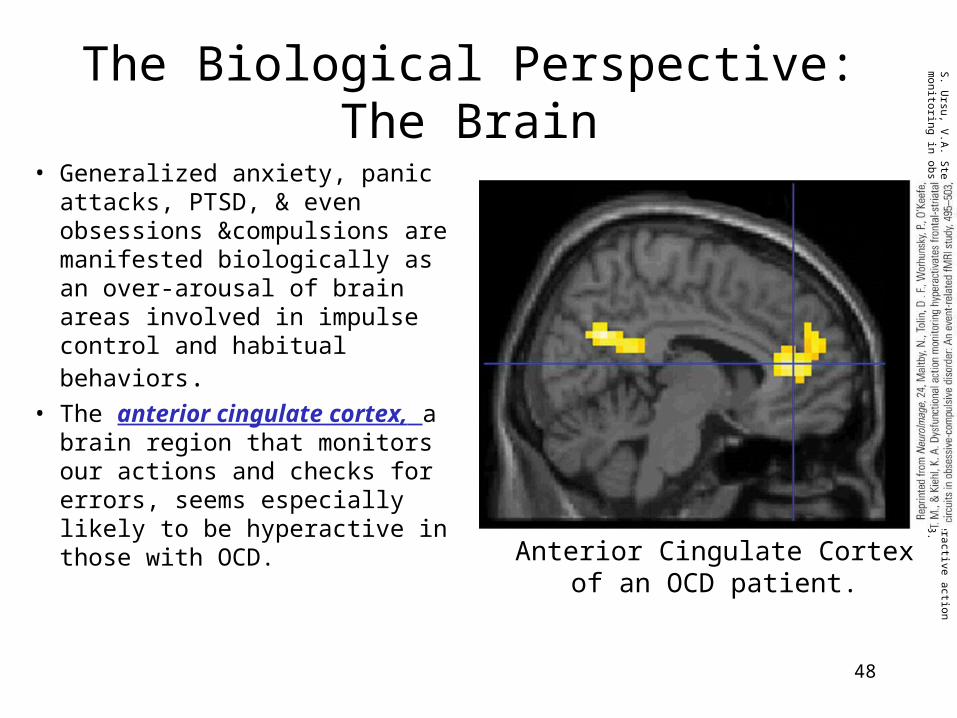
The Biological Perspective: The Brain
• Generalized anxiety, panic attacks, PTSD, & even obsessions &compulsions are manifested biologically as an over-arousal of brain areas involved in impulse control and habitual behaviors.
• The anterior cingulate cortex, a brain region that monitors our actions and checks for errors, seems especially likely to be hyperactive in those with OCD.
48
Anterior Cingulate Cortexof an OCD patient.
S. U
rsu, V.A
. Stenger, M
.K. S
hear, M.R
. Jones, & C
.S. Carter (2003). O
veractive action m
onitoring in obsessive-compulsive disorder. P
sychological Science, 14, 347-353.
49
Mood Disorders
Abnormal disturbances in emotion or mood.
Emotional extremes of mood disorders come in two principal forms.
1. Major depressive disorder2. Bipolar disorder
50
Dysthymic DisorderA milder form of major depression
•Dysthymic disorder lies between a blue mood and major depressive disorder. “ Down-in-the-dumps” mood that fills most of the day, nearly everyday. It can last for two or more years.•Chronic low energy•Low self-esteem•Difficulty concentrating & making decisions•May sleep and eat too much or too little
Major DepressiveDisorder
Blue Mood
DysthymicDisorder
51
Major Depressive Disorder
Depression is the “common cold” of psychological disorders. In a year, 5.8%
of men and 9.5% of women report depression worldwide (WHO, 2002).
Depression is the number one reason people seek mental health services and the leading cause of
disability worldwide.
52
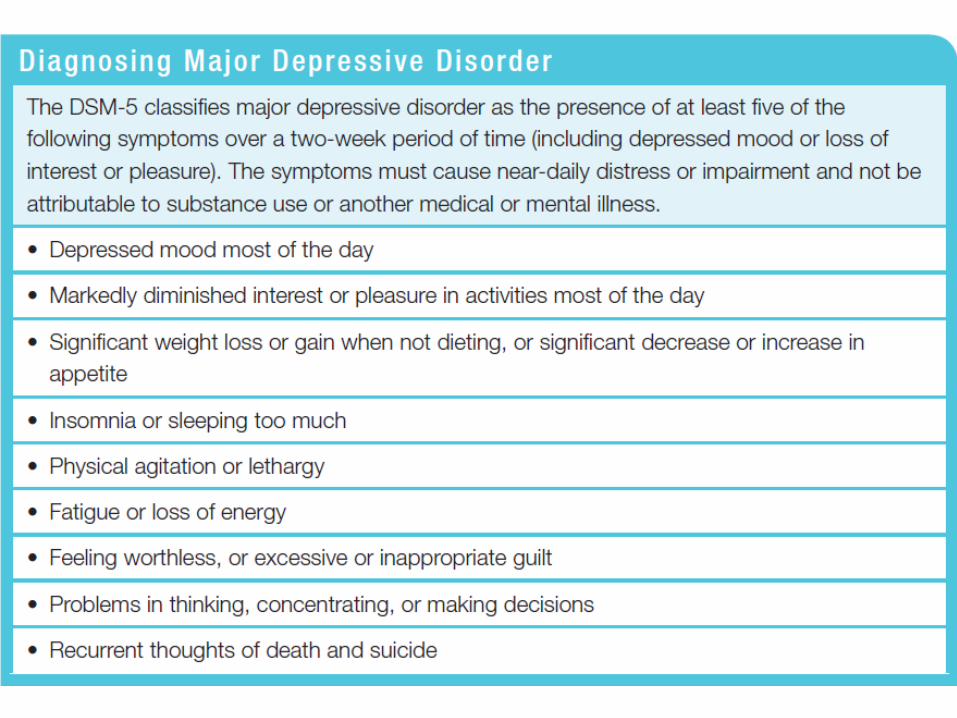
Major Depressive Disorder
Major depressive disorder occurs when signs of depression last two weeks or more and are
not caused by drugs or medical conditions.
1. Problems regulating appetite2. Problems regulating sleep3. Low energy4. Low self-esteem5. Difficulty concentrating and making
decisions6. Feelings of hopelessness
Signs include:
Treatments of Mood Disorders
• Selective serotonin reuptake inhibitors (SSRI’s)-antidepressant drugs
– Prozac, Zoloft
• Psychotherapy
54
55
Bipolar Disorder
• Formerly called manic-depressive disorder. An alternation between depression and mania signals bipolar disorder.
• Mania-hyperactive and wildly optimistic state.– Grandiose optimism and self esteem
is a symptom of the manic state.• Ex. Reckless investments, spending
sprees, and unsafe sex; they may find advice irritating.
Bipolar Disorder• Bipolar Disorder
– Mania (manic)
• Overtalkative, overactive, elated, little need for sleep, etc.
– Disruptive Mood Dysregulation Disorder-• Adolescent mood swings-rage to bubbly; emotional volatility
– Bipolar disorder and creativity• Composers, artists, poets, novelists and entertainers seem
especially prone
57
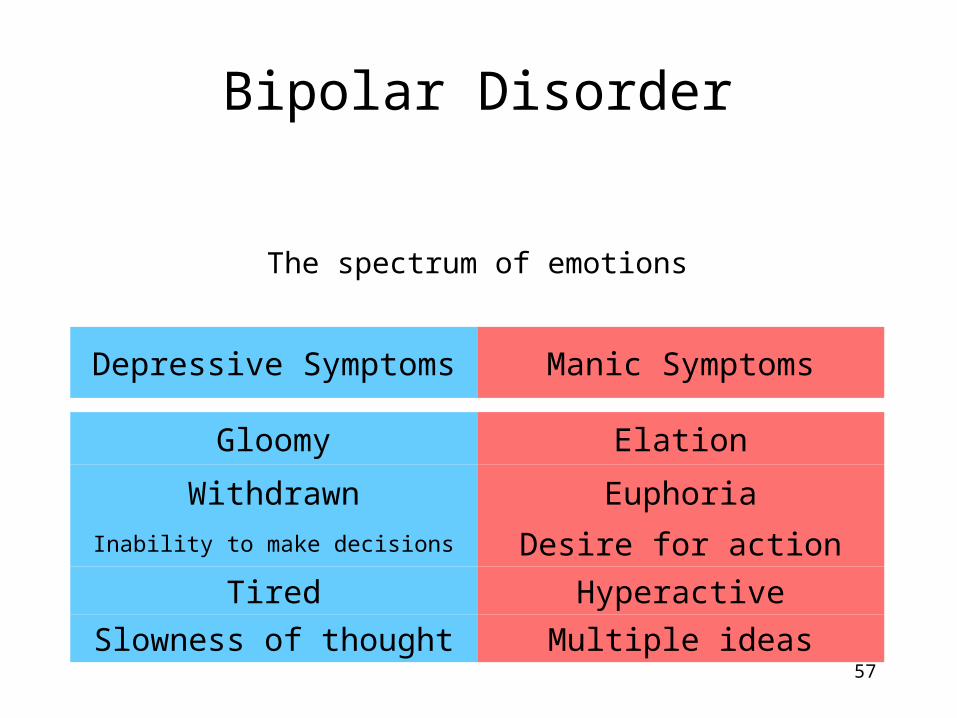
Bipolar Disorder
The spectrum of emotions
Multiple ideas
Hyperactive
Desire for action
Euphoria
Elation
Manic Symptoms
Slowness of thought
Tired
Inability to make decisions
Withdrawn
Gloomy
Depressive Symptoms
Treatment of Bipolar Disorder
• Lithium-a mood stabilizer that prevents the manic episodes (prevents neurons from being overstimulated)
• Lithium is often combined with antipsychotics and antidepressants.
58
Understanding Depressive and Bipolar Disorders
• Many behavioral and cognitive changes accompany depression
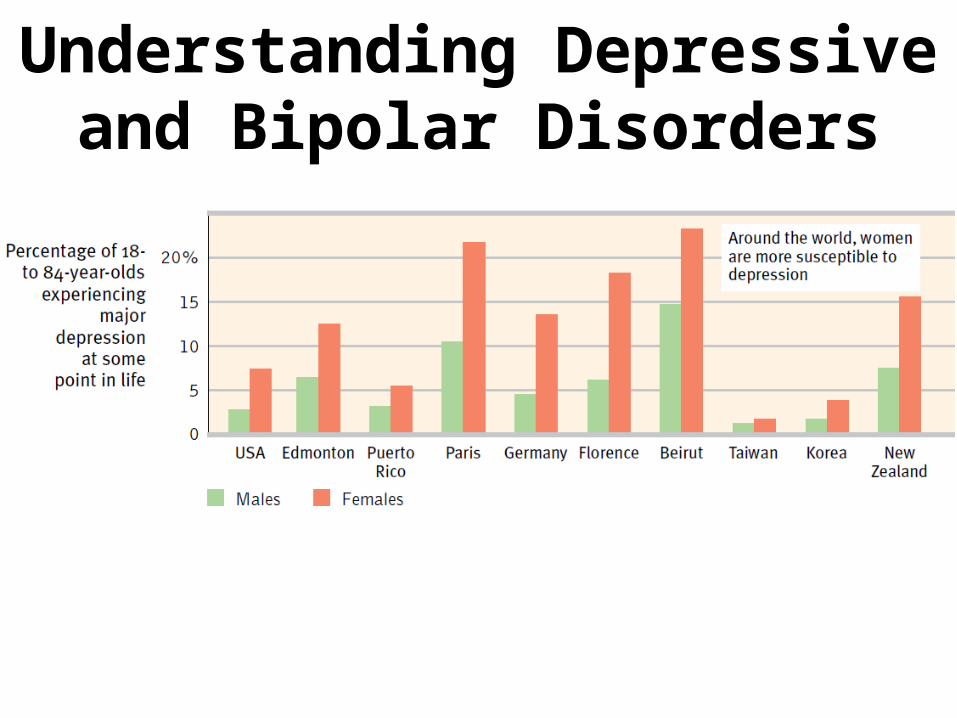
• Depression is widespread• Women’s risk of major depression is nearly
double men’s• Most major depressive episodes self-terminate• Stressful events related to work, marriage and
close relationships often proceed depression• With each new generation, depression is striking
earlier and affecting more people
Understanding Depressive and Bipolar Disorders
61
Biological Perspective
Genetic Influences: Mood disorders run in families. The rate of depression is higher in identical (50%) than fraternal twins (20%).
Linkage analysis and association studies link
possible genes and dispositions for
depression.
Jerry Irwin Photography
62
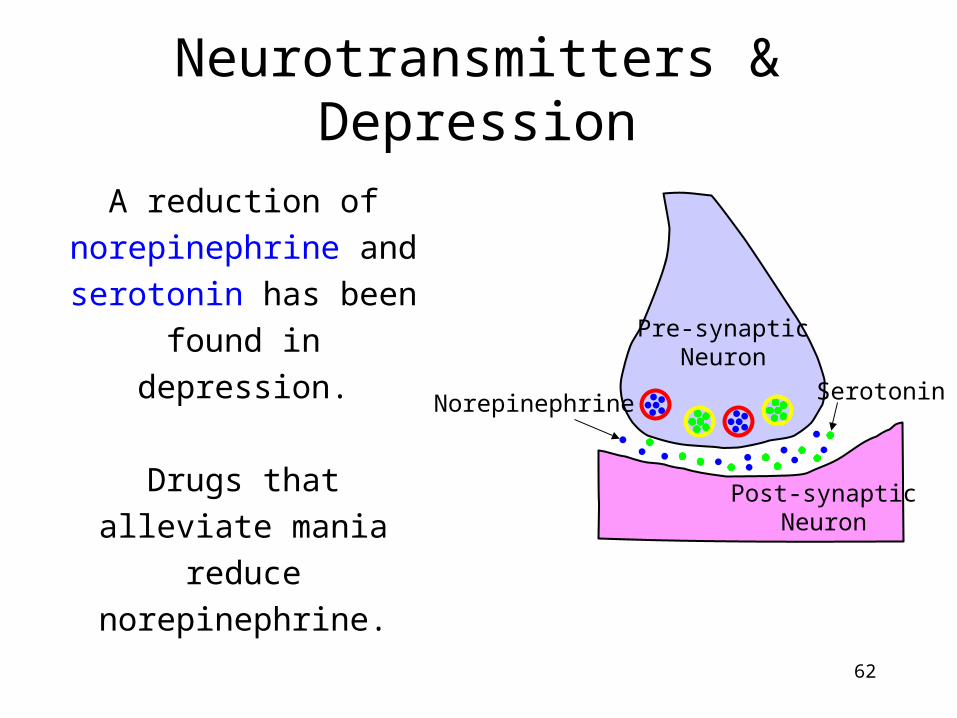
Neurotransmitters & Depression
Post-synapticNeuron
Pre-synapticNeuron
Norepinephrine Serotonin
A reduction of norepinephrine and serotonin has been
found in depression.
Drugs that alleviate mania reduce
norepinephrine.
63
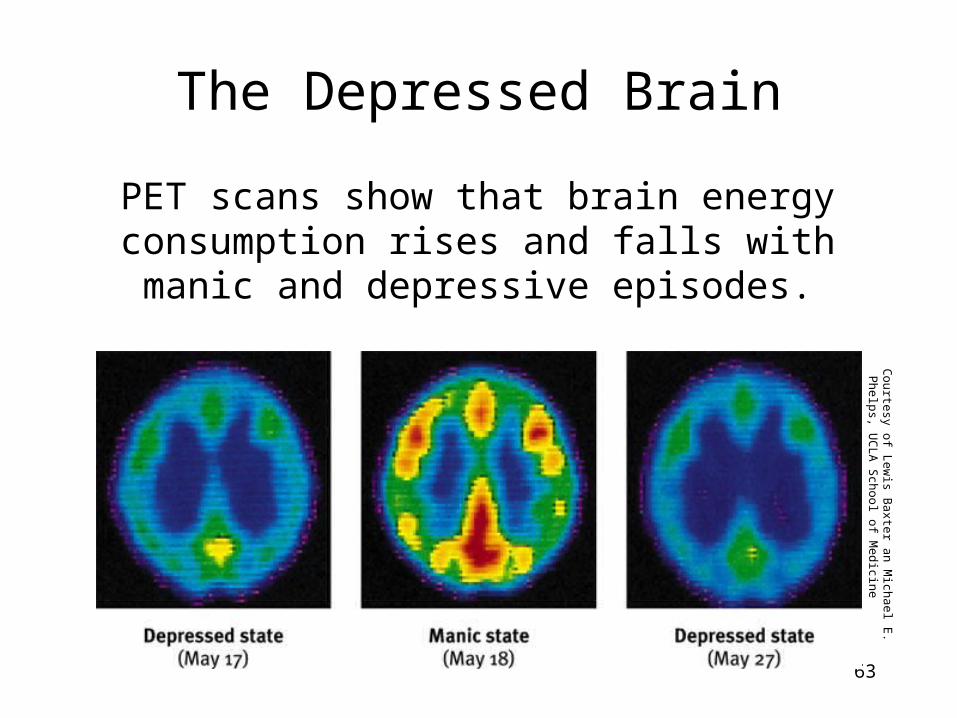
The Depressed Brain
PET scans show that brain energy consumption rises and falls with manic
and depressive episodes.
Courtesy of L
ewis B
axter an Michael E
. P
helps, UC
LA
School of M
edicine
64
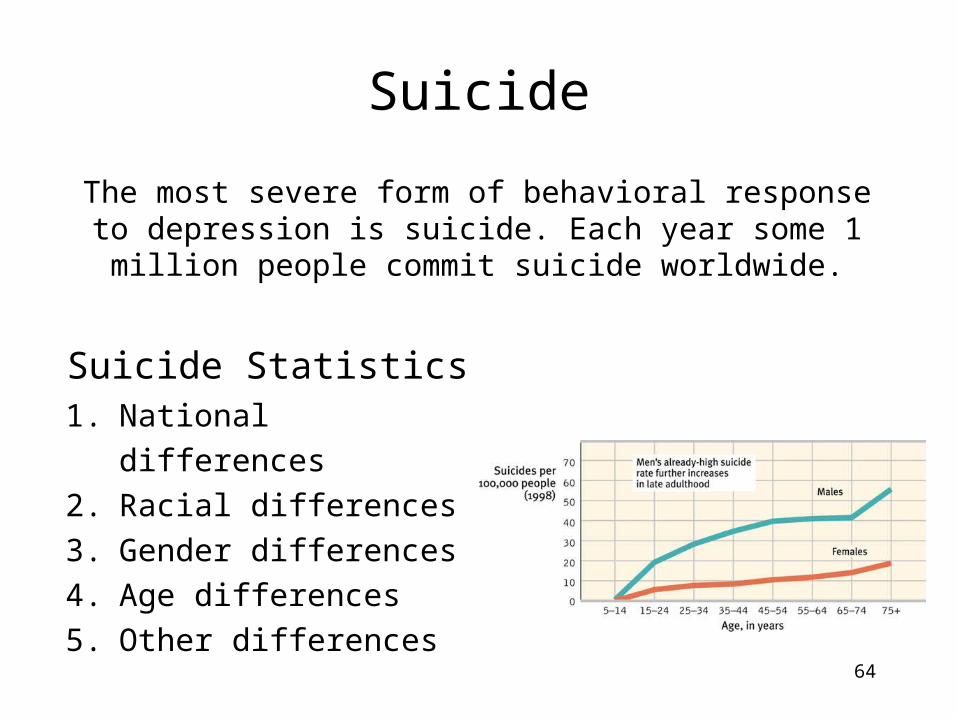
Suicide
The most severe form of behavioral response to depression is suicide. Each year some 1 million people commit suicide worldwide.
1. National differences2. Racial differences3. Gender differences4. Age differences5. Other differences
Suicide Statistics
65
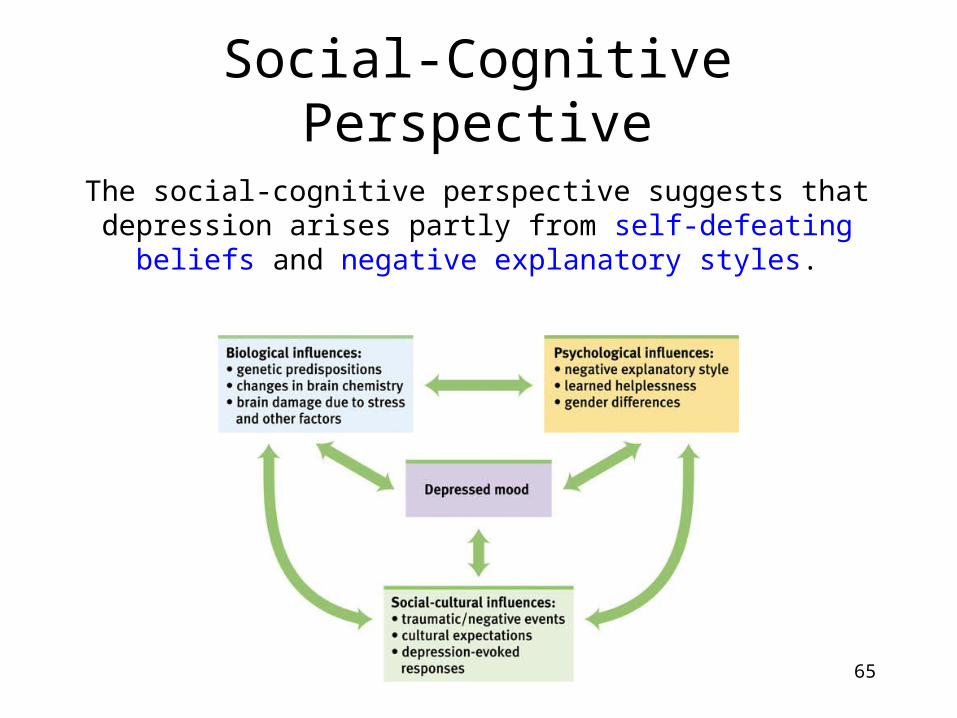
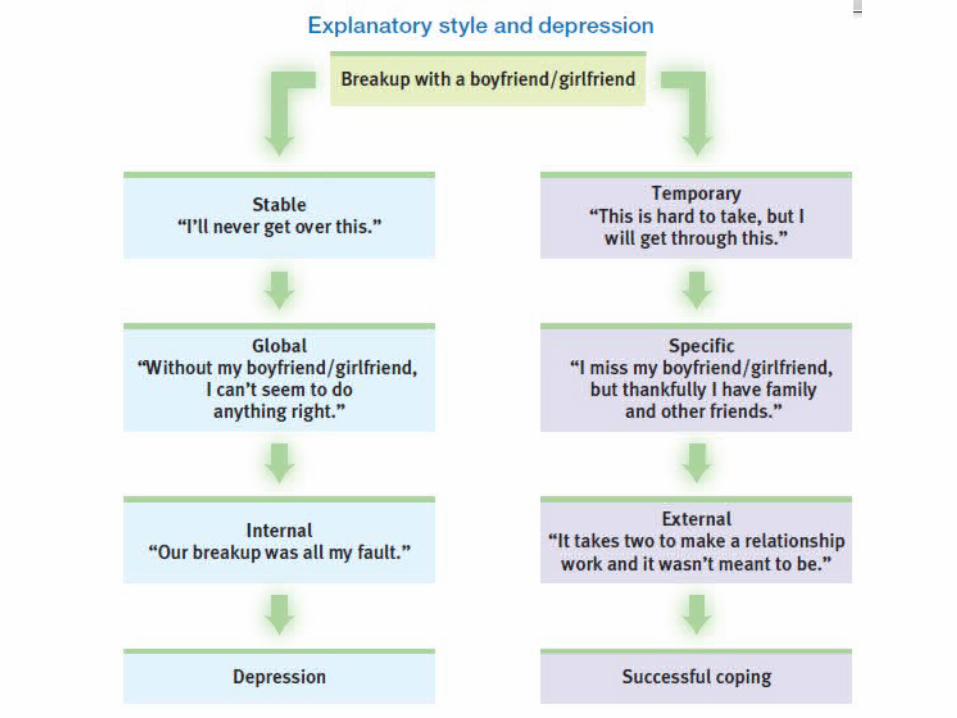
Social-Cognitive Perspective
The social-cognitive perspective suggests that depression arises partly from self-defeating
beliefs and negative explanatory styles.
Understanding Depressive and Bipolar Disorders
The Social-Cognitive Perspective
• Negative Thoughts and Moods Interact– Self-defeating beliefs
• Learned helplessness• Rumination- compulsive fretting; overthinking
about our problems– Explanatory style
• Stable, global, internal explanations– Cause versus indictor of depression?
68
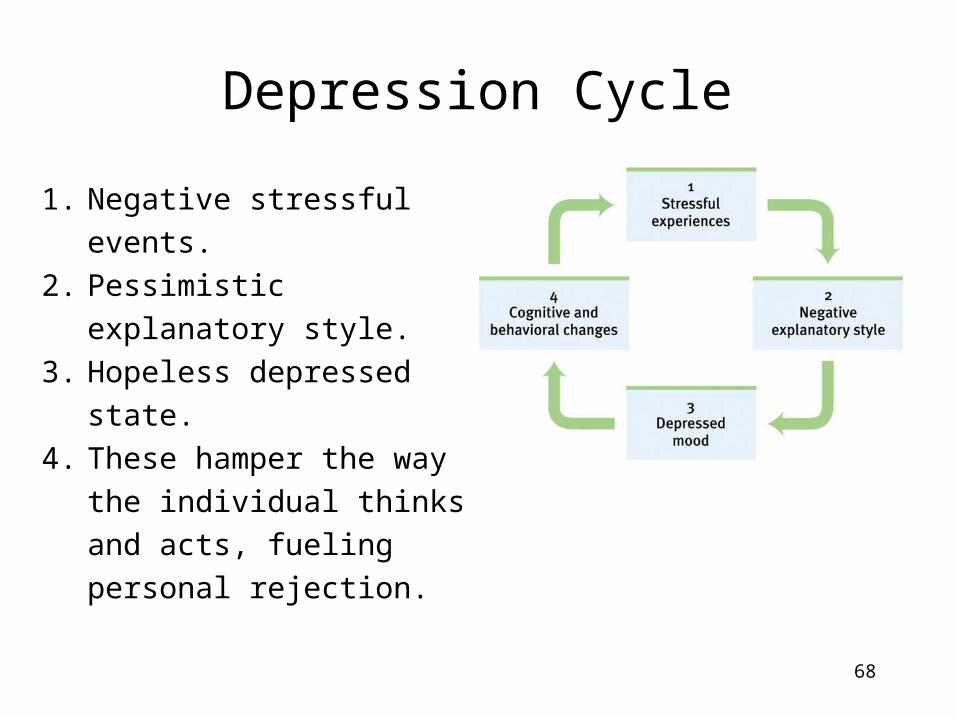
Depression Cycle
1. Negative stressful events.
2. Pessimistic explanatory style.
3. Hopeless depressed state.
4. These hamper the way the individual thinks and acts, fueling personal rejection.
Module 68:Schizophrenia Spectrum
70
Schizophrenia
If depression is the common cold of psychological disorders, schizophrenia is
the cancer.
Nearly 1 in a 100 suffer from schizophrenia (about 60 % men), and throughout the world over 24 million people suffer from this disease (WHO,
2011).
Schizophrenia strikes young people as they mature into adults. It affects men
and women equally, but men suffer from it more severely than women.
71
Symptoms of SchizophreniaThe literal translation is “split mind,”-not multiple
personalities, but a split from reality.A group of severe disorders characterized by the
following:
1. Disorganized and delusional thinking.
2. Disturbed perceptions. 3. Inappropriate emotions
and actions.Psychosis- a psychotic disorder marked by irrationality and lost contact with reality.
72
Other forms of delusions include, delusions of persecution (“someone is following me”)
or grandeur (“I am a king”).
Disorganized & Delusional Thinking
This morning when I was at Hillside [Hospital], I was making a movie. I was surrounded by movie stars … I’m Marry Poppins. Is this room painted blue to get me upset? My grandmother died four weeks after my eighteenth birthday.”
(Sheehan, 1982)
This monologue illustrates fragmented, bizarre thinking with distorted beliefs called delusions (“I’m Mary Poppins”).
73
Disorganized & Delusional Thinking
Many psychologists believe disorganized thoughts occur because of selective attention
failure (fragmented and bizarre thoughts).Word salad- jumbled ideas
74
Disturbed Perceptions
A schizophrenic person may perceive things that are not there (hallucinations). Frequently
such hallucinations are auditory and lesser visual, somatosensory, olfactory, or gustatory.
L. B
erthold, Untitled. T
he Prinzhorn Collection, U
niversity of Heidelberg
August N
atter, Witches H
ead. The Prinzhorn C
ollection, University of H
eidelberg
Photos of paintings by K
rannert Museum
, University of Illinois at U
rbana-Cham
paign
75
Inappropriate Emotions & Actions
A schizophrenic person may laugh at the news of someone dying or show no
emotion at all (apathy).
Patients with schizophrenia may continually rub an arm, rock a chair, or remain motionless for hours (catatonia).
76
Subtypes of Schizophrenia
Schizophrenia is a cluster of disorders. These subtypes share some features, but
there are other symptoms that differentiate these subtypes.
77
Positive and Negative Symptoms
Schizophrenics have inappropriate symptoms (hallucinations, disorganized
thinking, deluded ways) that are not present in normal individuals (positive symptoms).
Also known as Type I
Schizophrenics also have an absence of appropriate symptoms (apathy, expressionless faces, rigid bodies) that are present in normal
individuals (negative symptoms).Also known as Type II
78
Chronic and Acute Schizophrenia
When schizophrenia is slow to develop (chronic/process) recovery is doubtful.
Such schizophrenics usually display negative symptoms (Type II).
When schizophrenia rapidly develops (acute/reactive) recovery is better; responsive to drug therapy. Such schizophrenics usually
show positive symptoms (Type I).
79
Understanding Schizophrenia
Schizophrenia is a disease of the brain exhibited by the symptoms of the mind.
Dopamine Overactivity: Researchers found that schizophrenic patients express higher levels of dopamine D4 receptors in
the brain.
Brain Abnormalities
Abnormal Brain Activity
80
Paul T
hompson and A
rthur W. T
oga, UC
LA
Laboratory of N
euro Im
aging and Judith L. R
apport, National Institute of M
ental Health
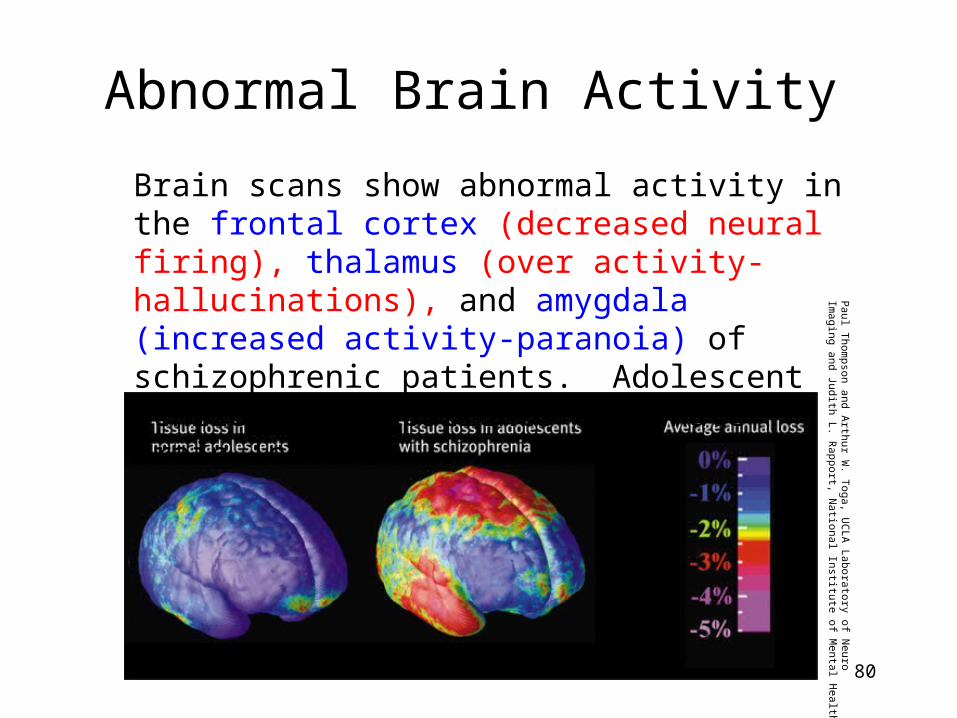
Brain scans show abnormal activity in the frontal cortex (decreased neural firing), thalamus (over activity-hallucinations), and amygdala (increased activity-paranoia) of schizophrenic patients. Adolescent schizophrenic patients also have brain lesions
81
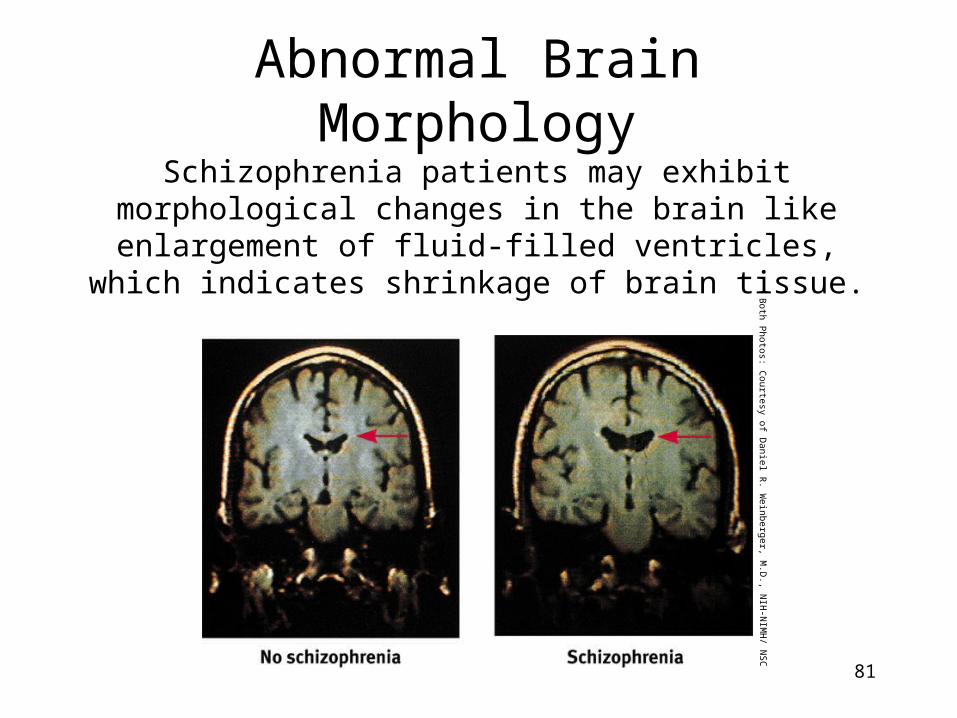
Abnormal Brain MorphologySchizophrenia patients may exhibit
morphological changes in the brain like enlargement of fluid-filled ventricles, which
indicates shrinkage of brain tissue.
Both Photos: C
ourtesy of Daniel R
. Weinberger, M
.D., N
IH-N
IMH
/ NSC
82
Viral Infection
• Schizophrenia has also been observed in individuals who contracted a viral infection (flu) during the middle of their fetal development.
Understanding Schizophrenia
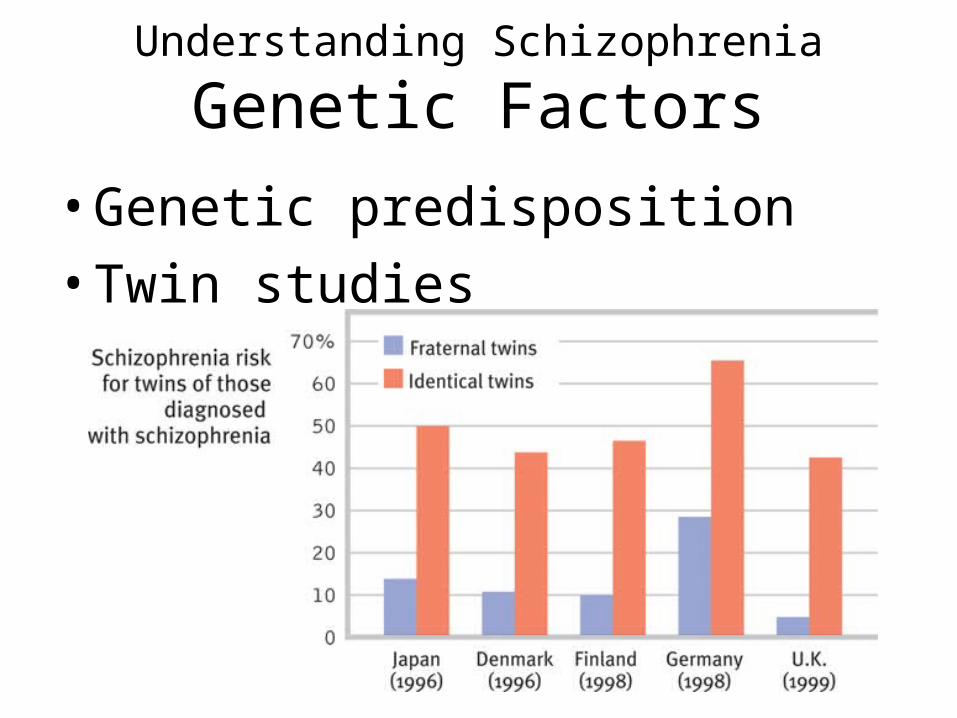
Genetic Factors
• Genetic predisposition
• Twin studies
84
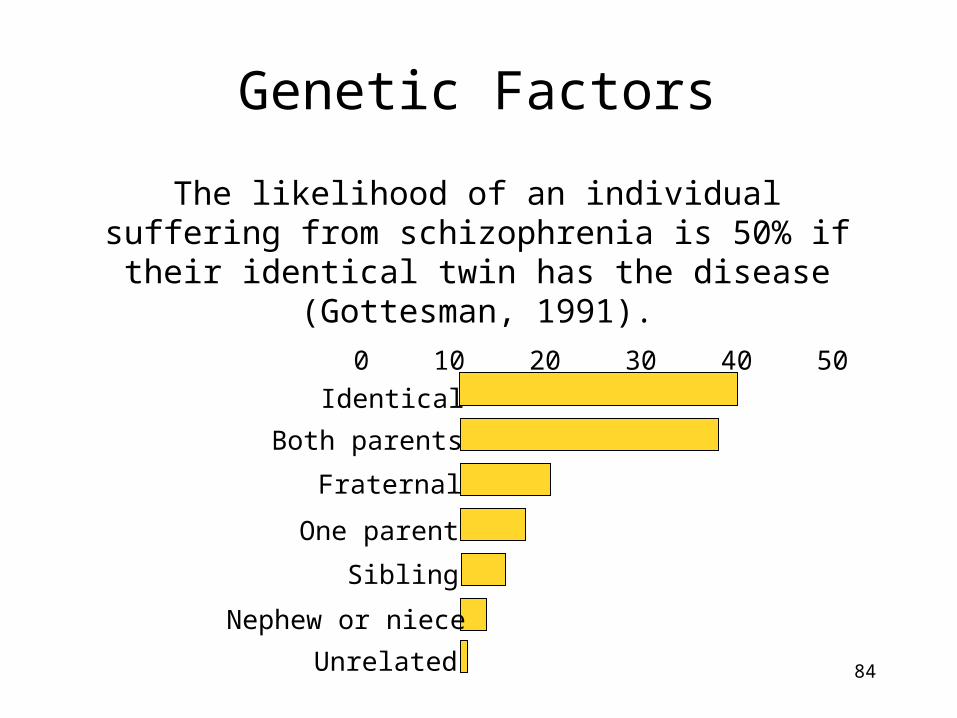
Genetic Factors
The likelihood of an individual suffering from schizophrenia is 50% if their identical
twin has the disease (Gottesman, 1991).
0 10 20 30 40 50Identical
Both parents
Fraternal
One parent
Sibling
Nephew or niece
Unrelated
85
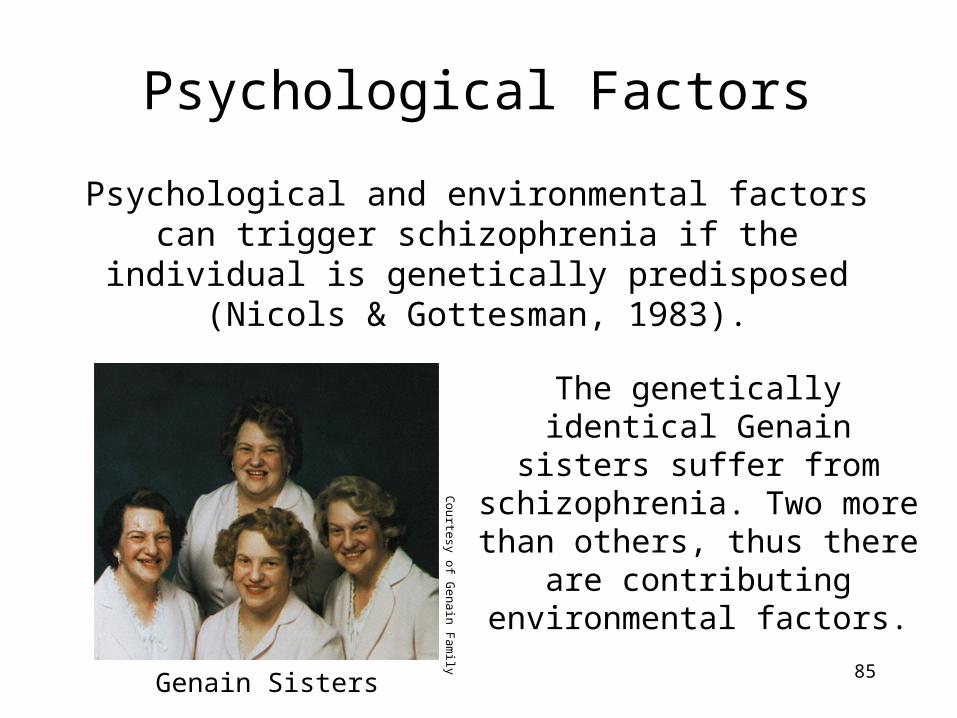
Psychological Factors
Psychological and environmental factors can trigger schizophrenia if the individual
is genetically predisposed (Nicols & Gottesman, 1983).
Genain Sisters
The genetically identical Genain
sisters suffer from schizophrenia. Two more
than others, thus there are contributing environmental
factors.
Courtesy of G
enain Fam
ily
Understanding Schizophrenia
Psychological Factors
• Possible warning signs– Mother severely schizophrenic– Birth complications (low weight/oxygen
deprivation)– Separation from parents– Short attention span– Disruptive or withdrawn behavior – Emotional unpredictability– Poor peer relations and solo play
Treatments for Schizophrenia
• Type I –Positive
– Typical neuroleptic drugs that reduce levels of dopamine.
– Mainly reduces the positive symptoms
– Ex. Thorazine
• Atypical neuroleptic drugs also reduce levels of dopamine and affects the amount of serotonin present.– These types of drugs
have some effects on negative symptoms.
– Clozapine
87
Module 69:Other Disorders
What are Somatoform Disorders?• A psychological disorder in which distressing
symptoms take a somatic (bodily) form without apparent physical causes.– Ex. Vomiting, prolonged pain, dizziness, blurred
vision, difficulty swallowing…– Conversion disorder- a rare type of somatoform
disorder in which a person experiences very specific genuine physical symptoms for which no physiological basis can be found• Ex. Paralysis or blindness
• Illness Anxiety Disorder– Formally known as hypochondriasis– People interpret normal sensations (a stomach
cramp today, a headache tomorrow) as symptoms of a dreaded disease.
89
Dissociative Disorder• A rare dissociative
disorder in which a person exhibits two or more distinct and alternating personalities. Formerly called multiple personality disorder.
• Conscious awareness becomes separated (dissociated) from previous memories, thoughts, and feelings.
• Symptoms– 1. Having a sense of
being unreal.– 2. Being separated from
the body.– 3. Watching yourself as
if in a movie.90
Dissociative Disorders
Understanding Dissociative Identity Disorder
• Genuine disorder or not?
• DID rates-between 1930-1960 only two per decade– In the 80’s the rates exploded to more
than 20,000
• Therapist’s creation– May reflect role-playing to therapists
suggestions
• May be a result of feelings of
anxiety
Feeding and Eating Disorders
• Eating disorders–Anorexia nervosa
–Bulimia nervosa
–Binge -eating disorder
Feeding and Eating Disorders
• Anorexia nervosa: an eating disorder in which a person (usually an adolescent female) maintains a starvation diet despite being significantly (15 percent or more) underweight.– Usually begins as a weight-loss diet
– People with anorexia—usually adolescents and 9 times out of 10 females—drop significantly below normal weight.
– They feel fat, fear being fat, and remain obsessed with losing weight, and sometimes exercise excessively.
– About half of those with anorexia display a binge-purge-depression cycle.
93
Feeding and Eating Disorders
• Bulimia nervosa: an eating disorder in which a person alternates binge eating (usually of high-calorie foods) with purging (by vomiting or laxative use) or fasting.
• Binge-purge eaters—mostly women in their late teens or early twenties—eat in spurts, sometimes influenced by friends who are bingeing (Crandall, 1988).
• Unlike anorexia, bulimia is marked by weight fluctuations within or above normal ranges, making the condition easy to hide.
94
Feeding and Eating Disorders
• Binge-eating disorder: significant binge-eating episodes, followed by distress, disgust, or guilt, but without the compensatory purging or fasting that marks bulimia nervosa.
• A national study funded by the U.S. National Institute of Mental Health reported that, at some point during their lifetime:– 0.6 percent of people meet the criteria for anorexia,– 1 percent for bulimia, and – 2.8 percent for binge-eating disorder
95
So, how can we explain these disorders?
• Mothers of girls with eating disorders tend to focus on their own weight and on their daughters’ weight and appearance (Pike & Rodin, 1991).
• Families of bulimia patients have a higher-than-usual incidence of childhood obesity and negative self-evaluation (Jacobi et al., 2004).
• Families of anorexia patients tend to be competitive, high-achieving, and protective (Pate et al., 1992; Yates, 1989, 1990)
• Low self esteem/evaluation• Genetics• Cultural influences
96
97
Personality Disorders
Personality disorders are disruptive, inflexible and enduring behavior patterns that impair one’s social functioning. They are three clusters of personality disorders:
A-Eccentric/odd behaviorB- Dramatic/impulsive behaviors C-Anxiety
Personality Disorders Cluster A-Odd/Eccentric
– Schizoid PD- expresses eccentric behaviors such as emotionless disengagement
Cluster B- Dramatic/Impulsive– Histrionic PD-exhibits dramatic or impulsive behaviors;
shallow, attention-getting emotions and goes to great lengths to gain others praise and reassurance.
– Narcissistic PD- exaggerates their own importance, aided by fantasies. They find criticism hard to accept, often reacting with rage or shame.
– Antisocial personality disorder Cluster C-Anxiety/Fearful
– Avoidant PD- expresses anxiety, such as fearful sensitivity to rejection.
99
Antisocial Personality Disorder-Cluster B
Sometimes called a sociopath or psychopath.A disorder in which the person (usually men) exhibits a lack of conscience for wrongdoing, even toward friends and family members. May be aggressive and ruthless or a clever con artist.
Symptoms include: lies, steals, fight, display unrestrained sexual behavior
They feel and fear little. They express little regret over violating others’ rights. Lack of conscience becomes plain before age 15. Despite their remorseless and sometimes criminal
behavior, criminality is not an essential component of antisocial behavior (Skeem & Cooke, 2010).
100
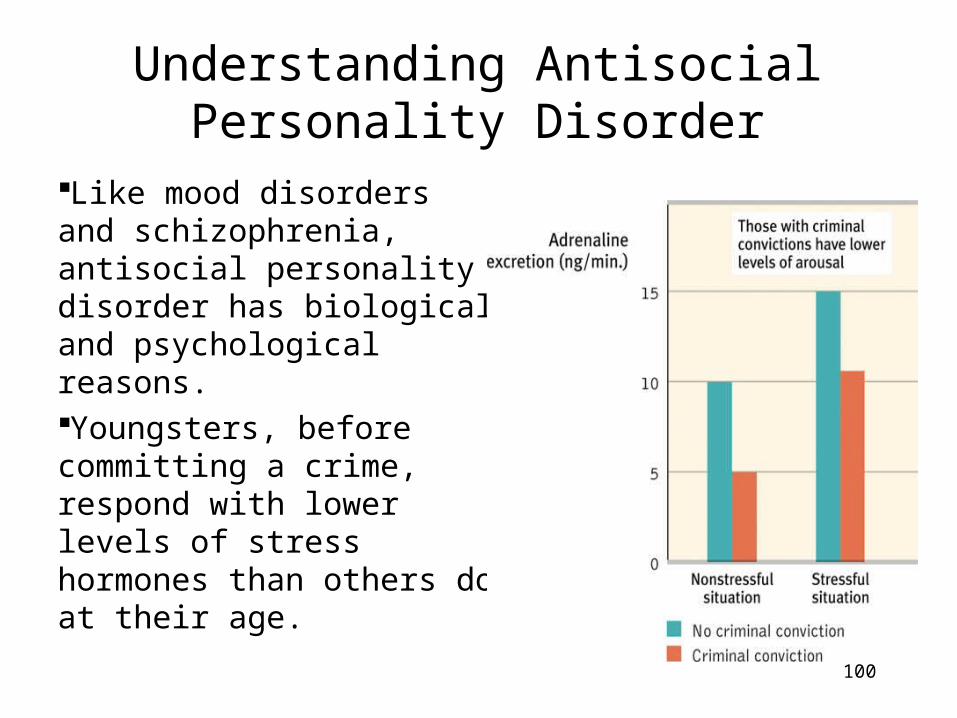
Understanding Antisocial Personality Disorder
Like mood disorders and schizophrenia, antisocial personality disorder has biological and psychological reasons. Youngsters, before committing a crime, respond with lower levels of stress hormones than others do at their age.
101
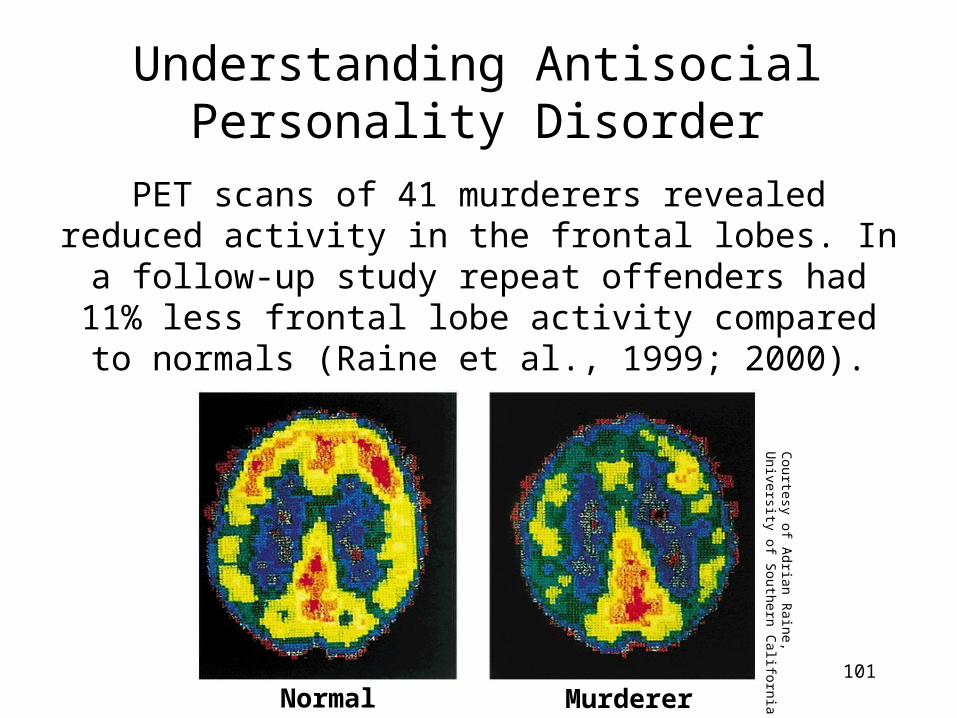
Understanding Antisocial Personality Disorder
PET scans of 41 murderers revealed reduced activity in the frontal lobes. In a follow-up
study repeat offenders had 11% less frontal lobe activity compared to normals (Raine et
al., 1999; 2000).
Normal Murderer
Courtesy of A
drian Raine,
University of Southern C
alifornia
102
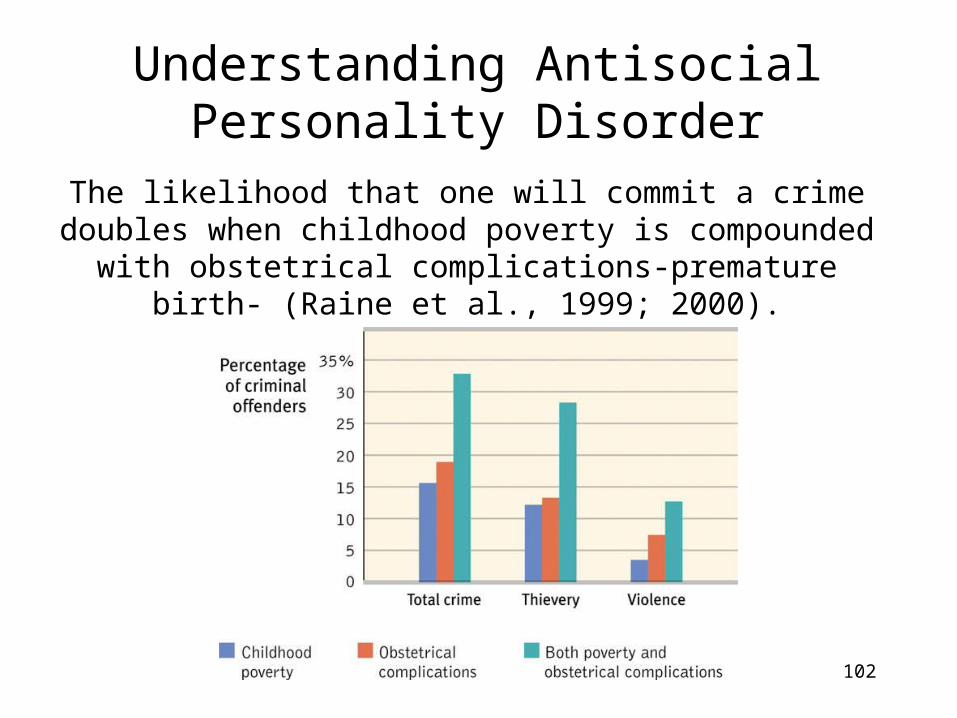
Understanding Antisocial Personality Disorder
The likelihood that one will commit a crime doubles when childhood poverty is compounded with
obstetrical complications-premature birth- (Raine et al., 1999; 2000).
Developmental Disorders• Autism-characterized by disabilities in language, social
interaction, the ability to understand another person’s state of mind, cognitive development and repetitive behavior
• Occurs in about 1 in 500 children and often is first suspected at about 1.5-2 years of age, when the child fails to develop language.– Most experts believe it is a brain disorder with a
genetic basis.
• Asperger’s Syndrome- high functioning autism; children with high intelligence have deficits in social interaction.
103
104
Rates of Psychological Disorders
105
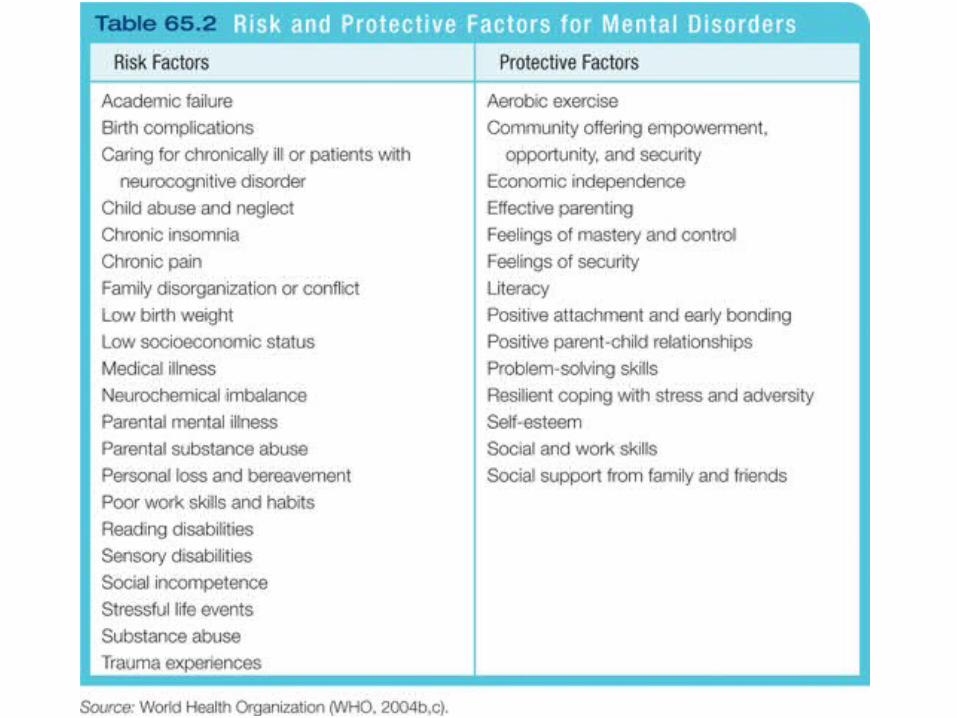
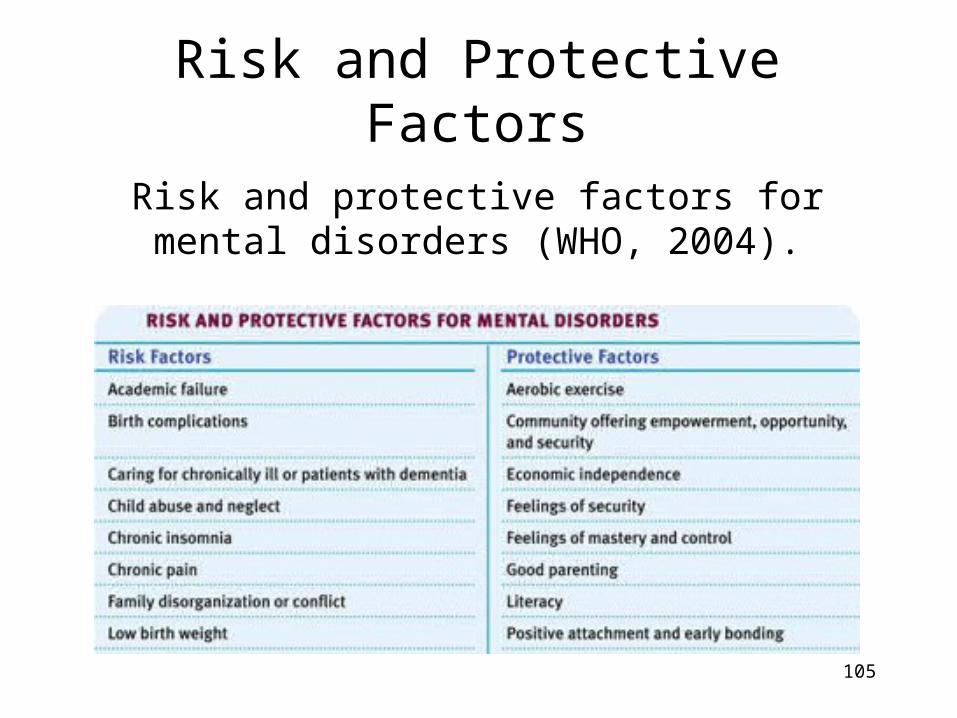
Risk and Protective Factors
Risk and protective factors for mental disorders (WHO, 2004).
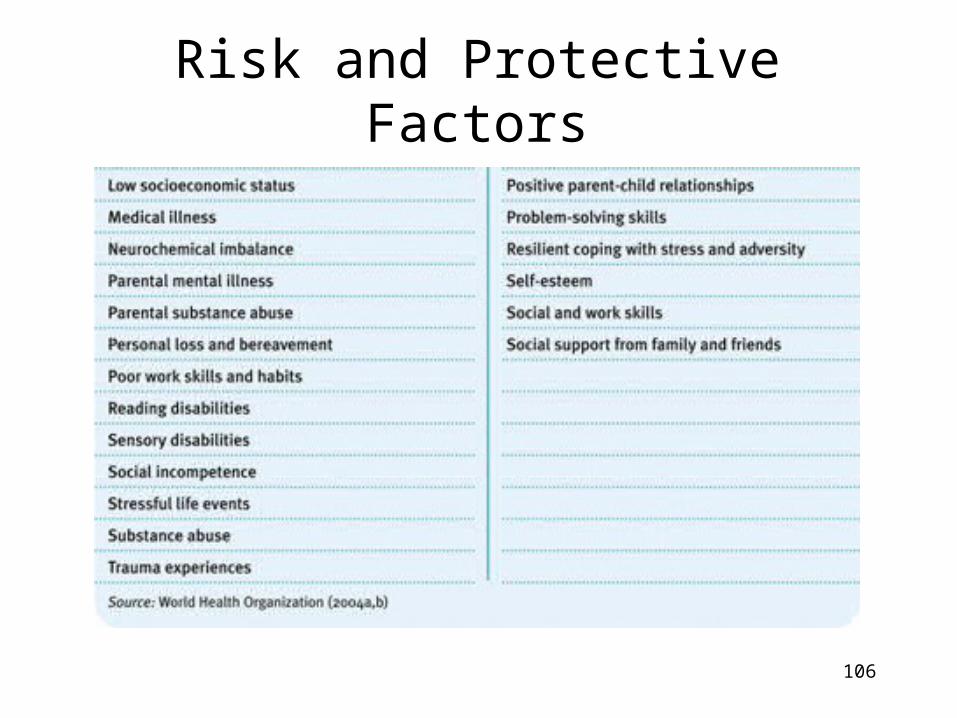
106
Risk and Protective Factors